Carotid Intima-Media Thickness (CIMT) measurement via high-resolution B-mode ultrasound is a non-invasive, validated method for assessing subclinical atherosclerosis and predicting future cardiovascular events. The image provided displays a longitudinal view of the left proximal common carotid artery (CCA) captured using a Samsung HS70A ultrasound system. This modality allows clinicians to visualize the arterial wall architecture with precision, identifying early structural changes before they manifest as obstructive plaques or clinical symptoms such as stroke or myocardial infarction.
Label-by-Label Explanation
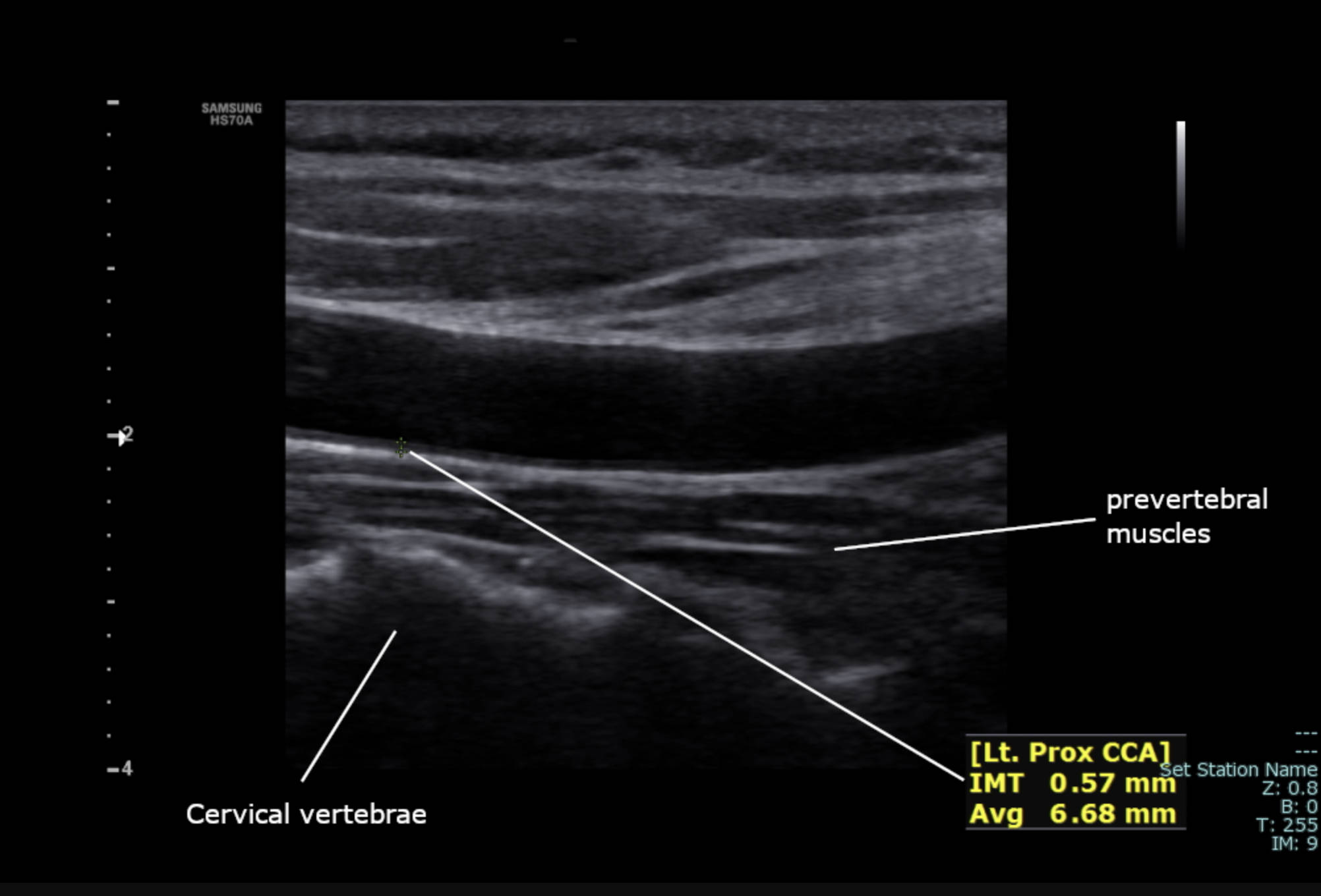
Cervical vertebrae: These are the bony structural elements of the neck located deep to the carotid sheath. In this ultrasound image, the vertebral surface appears as a bright, hyperechoic line that creates a distinct acoustic shadow, effectively blocking the transmission of sound waves to deeper structures.
prevertebral muscles: This layer of soft tissue sits between the posterior wall of the carotid artery and the cervical spine. Identifying these muscles helps the sonographer confirm the longitudinal orientation of the probe and ensures that the vessel being imaged is indeed the carotid artery rather than a more superficial structure.
Lt. Prox CCA: This label specifies the anatomical region being scanned: the left proximal common carotid artery. The proximal segment is located closer to the aortic arch (on the left) or the brachiocephalic trunk (on the right) and is a standard site for screening for early atherosclerotic changes.
IMT 0.57 mm: This value represents the measurement of the Intima-Media Thickness, which is the combined thickness of the innermost two layers of the arterial wall. A measurement of 0.57 mm in this patient is well within the healthy physiological range, as values exceeding 0.8 mm or 0.9 mm often suggest an increased risk for cardiovascular disease.
Avg 6.68 mm: This indicates the average internal diameter of the carotid lumen at the site of measurement. Monitoring the luminal diameter is important for detecting arterial remodeling, where the vessel may enlarge to compensate for wall thickening, or narrow in the presence of advanced stenosis.
Anatomical Considerations in Carotid Ultrasound
The common carotid artery is housed within the carotid sheath, a dense layer of fascia that also contains the internal jugular vein and the vagus nerve. In a longitudinal ultrasound section, the artery appears as an anechoic (black) tubular structure due to the fluid nature of blood. The surrounding tissues, including the thyroid gland medially and the sternocleidomastoid muscle superficially, provide essential landmarks for the sonographer.
When performing CIMT measurements, it is standard practice to focus on the “far wall” of the artery—the wall furthest from the transducer. This is because the physics of ultrasound reflection at the media-adventitia interface on the far wall produces a sharper image, known as the double-line sign. This sign consists of two parallel echogenic lines separated by a hypoechoic space, representing the intima-lumen interface and the media-adventitia interface respectively.
The Pathophysiological Significance of CIMT
The development of atherosclerosis is a gradual process that often begins decades before a clinical event occurs. The earliest detectable change is the thickening of the intima-media layer, driven by lipid accumulation, inflammatory cell infiltration, and smooth muscle cell proliferation. CIMT serves as a surrogate marker for the total systemic atherosclerotic burden.
Research has shown that for every 0.1 mm increase in carotid IMT, the risk of myocardial infarction increases by approximately 10-15%, and the risk of stroke increases by 13-18%. Because ultrasound is radiation-free and relatively inexpensive, it is an ideal tool for longitudinal monitoring of patients with metabolic syndrome, hypertension, or a strong family history of heart disease.
Educational Importance for Healthcare Providers
For medical students and radiology residents, mastering the identification of these neck landmarks is fundamental. Distinguishing the CCA from the internal jugular vein is the first step; while the artery is pulsatile and non-compressible, the vein is easily compressed with light transducer pressure and exhibits respiratory variations. Furthermore, recognizing the depth of the cervical vertebrae and prevertebral muscles ensures that the depth settings on the ultrasound machine are optimized for the best resolution of the arterial wall.
Understanding the difference between a simple intimal thickening and a discrete plaque is also vital. A plaque is generally defined as a focal structure protruding into the arterial lumen that is at least 0.5 mm thicker than the surrounding IMT, or a structure with a total thickness greater than 1.5 mm. Correctly labeling and measuring these features allows for accurate risk stratification and informs preventative management strategies.
Summary
Carotid ultrasound is a powerful diagnostic tool that bridges the gap between anatomy and clinical pathology. The measurement of an IMT of 0.57 mm in the left proximal CCA, as shown in this image, provides a snapshot of a healthy vascular wall. By observing the spatial relationship between the artery, the prevertebral muscles, and the underlying vertebrae, clinicians can reliably assess vascular health. Regular training in ultrasound landmarks and measurement techniques is essential for accurate cardiovascular risk assessment in modern clinical practice.
Medical Learning Tips
- The double-line sign on ultrasound represents the interfaces of the intima and media layers against the lumen and adventitia.
- CIMT measurements should ideally be performed on the far wall of the artery for maximum diagnostic accuracy.
- A CIMT value above 0.9 mm is typically considered a sign of increased cardiovascular risk across most adult populations.


{kind=link}