A lung cavity is defined as a gas-filled space within a zone of pulmonary consolidation, a mass, or a nodule, occurring as a result of focal tissue necrosis. In clinical practice, identifying a cavitary lesion on a chest radiograph is a critical finding that significantly narrows the differential diagnosis. This image demonstrates a classic presentation of cavitary lung disease, primarily affecting the right upper lobe, which provides essential visual cues for medical learners regarding the severity and distribution of pulmonary infections or malignancies. Understanding the morphology and location of these lesions is paramount for guiding further diagnostic investigations and therapeutic interventions.
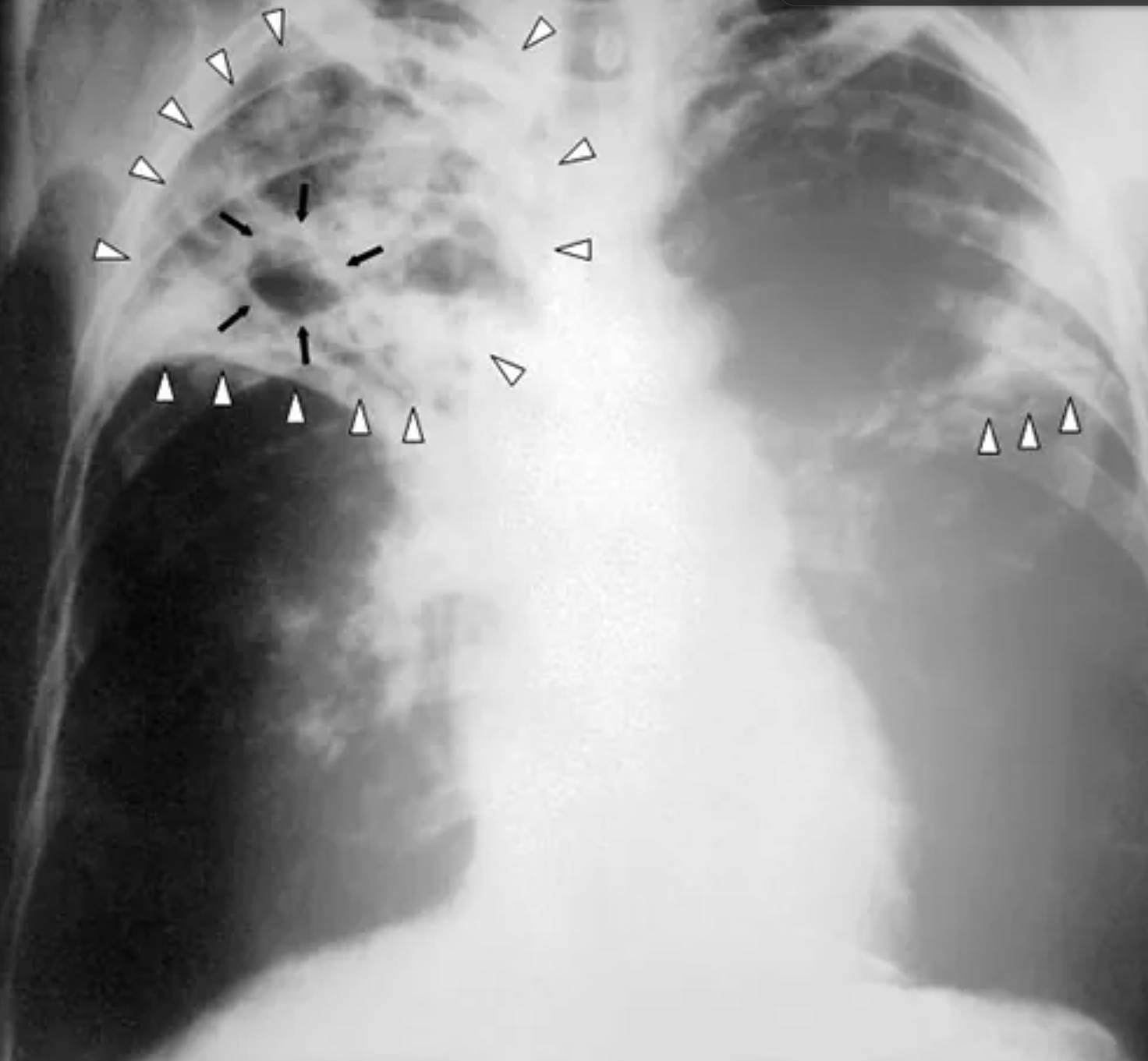
Image Overview
The radiograph presented is a posterior-anterior (PA) view of the chest showing a large, irregular radiolucent area in the right upper lobe. This central clearing, highlighted by multiple black arrows, represents a lung cavity. This cavity is surrounded by dense, heterogeneous opacities, often termed consolidation, which are indicated by the white open arrowheads. These arrowheads also track along the periphery of the upper right lung and appear in the contralateral mid-lung field, suggesting a multifocal or potentially bilateral pathological process.
The solid white arrowheads mark the inferior boundary of the primary consolidative process in the right upper lobe, which appears to align with the horizontal fissure. The overall radiological appearance is highly suggestive of a chronic inflammatory or infectious process that has progressed to the point of significant tissue destruction, resulting in the formation of air-filled voids within the lung parenchyma. The lack of a clear air-fluid level within the cavity suggests that the necrotic debris has been mostly expectorated through the bronchial tree.
Pathogenesis of Lung Cavitation
Cavitation occurs when necrotic lung tissue is expelled into the tracheobronchial tree, leaving behind an air-filled space. This process typically begins with a focus of infection or injury that leads to localized cell death. In the context of pyogenic bacterial infections, the release of proteolytic enzymes by neutrophils results in liquefactive necrosis, which rapidly breaks down the lung architecture. If this material drains into a bronchus, a cavity is formed.
In granulomatous diseases like tuberculosis, the body’s immune response creates a localized area of caseous necrosis. When this necrotic center liquefies and establishes communication with an airway, the solid debris is cleared, and air replaces it, creating the radiolucent appearance seen on the X-ray. The thickness and regularity of the cavity wall are critical features for the radiologist; while this image shows a moderately thick wall, very thick or nodular walls are often associated with malignancy, whereas thin, smooth walls may indicate a resolving abscess or a chronic cyst.
Differential Diagnosis of Cavitary Lesions
The identification of a cavity in the upper lobe of the lung should immediately prompt a structured differential diagnosis. The anatomical preference of certain pathogens for the upper lobes is often related to higher oxygen tension and reduced lymphatic drainage in these regions. The most common considerations include:
- Pulmonary Tuberculosis: Characteristically involves the apical and posterior segments of the upper lobes. Cavitation is a hallmark of reactivation (post-primary) TB and indicates high infectivity.
- Necrotizing Pneumonia and Lung Abscess: Often caused by anaerobic bacteria or Staphylococcus aureus. These usually present with more acute symptoms and may show air-fluid levels.
- Fungal Infections: Pathogens such as Aspergillus can cause cavitation or inhabit pre-existing cavities, forming a mycetoma (fungal ball).
- Malignancy: Primary lung cancers, particularly squamous cell carcinoma, frequently undergo central necrosis. These typically present as thick-walled cavities with irregular internal margins.
- Autoimmune Disease: Conditions like granulomatosis with polyangiitis can cause multiple cavitating nodules throughout the lungs.
Clinical and Radiological Correlation
Interpreting a chest radiograph requires tight correlation with the patient’s clinical history. For instance, a patient with a chronic cough, weight loss, and night sweats paired with this image would be managed as a suspected case of tuberculosis until proven otherwise. In contrast, an acute onset of fever and foul-smelling sputum would favor a pyogenic abscess. The bilateral nature of the infiltrates seen here, marked by the open arrowheads in both the right and left lung zones, suggests a more disseminated or advanced stage of disease.
Furthermore, the presence of the horizontal fissure (demarcated by the solid white arrowheads) being pulled superiorly or appearing highly distinct can indicate volume loss in the upper lobe, a common feature of chronic fibrocavitary diseases. Clinicians must also look for secondary signs, such as hilar lymphadenopathy or pleural effusions, which can provide additional clues to the underlying etiology.
Educational and Diagnostic Significance
For healthcare learners, this image serves as a fundamental example of how to distinguish between different radiographic densities. The contrast between the black radiolucency of the cavity and the white radiopacity of the surrounding consolidation illustrates the loss of lung tissue. Mastery of these patterns allows for the early implementation of life-saving measures, such as respiratory isolation in the case of suspected tuberculosis, which prevents further transmission in hospital and community settings.
While the chest X-ray is the initial screening tool, high-resolution CT (HRCT) is often the next step in evaluating cavitary lesions. HRCT can provide a much clearer view of the wall thickness, the presence of internal debris, and the presence of “tree-in-bud” opacities, which are highly suggestive of the endobronchial spread of infection. Recognizing these patterns on a plain film is the first step in a complex diagnostic journey that includes sputum cultures, molecular testing, and sometimes tissue biopsy.
Summary
The formation of a lung cavity is a significant radiological finding indicating tissue necrosis and communication with the airway. This PA chest radiograph highlights a prominent cavity in the right upper lobe surrounded by consolidation, a pattern typical of severe infectious processes like tuberculosis or necrotizing pneumonia. By analyzing the location, wall characteristics, and associated lung findings, clinicians can effectively prioritize diagnostic tests and initiate appropriate treatment early in the disease course.
Medical Learning Tips
- Always measure the wall thickness of a cavity, as walls thicker than 15 mm significantly increase the likelihood of malignancy.
- Upper lobe cavitation is a classic radiological sign of reactivation tuberculosis due to the high oxygen tension in those lung segments.
- The presence of an air-fluid level within a cavity suggests a communication with the bronchus and the presence of infected liquid or blood.


{kind=link}