The human skin is the body’s largest organ, serving as a complex and dynamic barrier that protects internal systems from environmental stressors, pathogens, and mechanical injuries. The outermost region of the skin, known as the epidermis, is a stratified squamous epithelium that undergoes a continuous process of renewal and maturation. Understanding the histological structure of this tissue is fundamental for medical professionals and students alike, as it provides the foundation for diagnosing various dermatological conditions. By examining the layers of the epidermis under a microscope, we can observe the fascinating transition of cells as they migrate from the deep proliferative zone to the surface, where they eventually form a tough, water-resistant shield. This article delves into the specific characteristics of each epidermal layer and explores the physiological processes that maintain skin integrity and health.
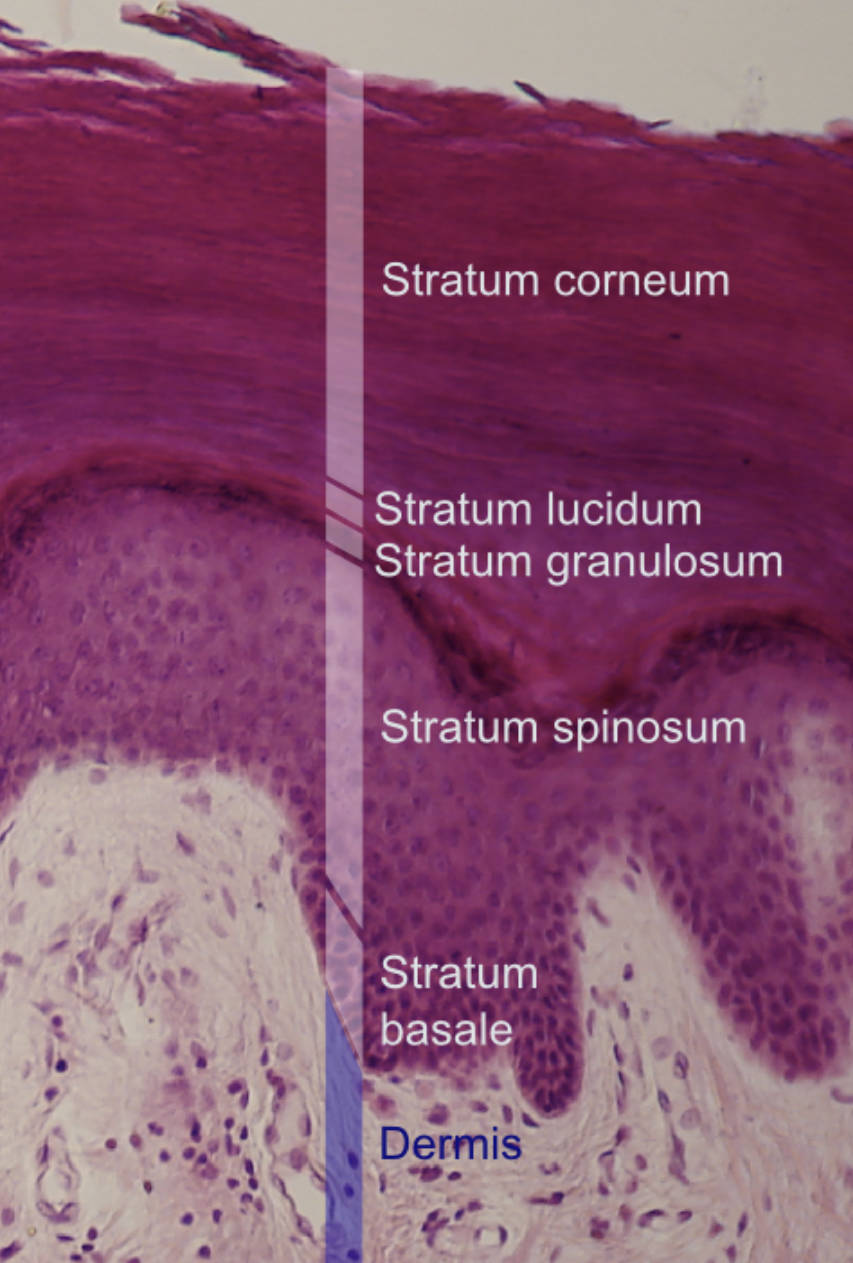
Stratum corneum: This is the most superficial layer of the epidermis, consisting of multiple rows of dead, flattened keratinocytes called corneocytes. These cells are filled with tough keratin and lack nuclei, acting as the primary physical barrier against dehydration and microbial invasion.
Stratum lucidum: Visible as a thin, translucent band, this layer is exclusively found in “thick skin,” such as the palms of the hands and soles of the feet. It contains dead cells filled with eleidin, a clear protein that is an intermediate product in the formation of keratin.
Stratum granulosum: This layer marks the transition between the deeper active layers and the superficial dead layers of the skin. Cells here contain dense keratohyalin granules and lamellar granules, which release lipids to create a waterproof barrier for the skin.
Stratum spinosum: Often referred to as the prickly layer, it is comprised of several layers of polyhedral cells held together by strong desmosomes. When tissue is prepared for microscopy, the cells shrink, making these attachments look like tiny spines protruding from the cell surface.
Stratum basale: This is the deepest single layer of the epidermis, sitting directly on the basement membrane that separates it from the dermis. It consists of actively dividing stem cells that produce new keratinocytes, as well as melanocytes responsible for skin pigmentation.
Dermis: Although situated below the epidermis, the dermis is critical for skin function as it houses the blood vessels that provide nutrients via diffusion. This connective tissue layer also contains sensory receptors, hair follicles, and sweat glands that support the overlying epithelium.
The Cellular Dynamics of the Epidermal Barrier
The primary cell type found within the layers of the epidermis is the keratinocyte, which produces the fibrous protein keratin. The life cycle of a keratinocyte begins in the stratum basale and concludes when it is shed from the stratum corneum in a process called desquamation. This journey typically takes approximately four weeks in a healthy individual. During this migration, the cells undergo profound biochemical changes, transforming from metabolically active cuboidal cells into flattened, lifeless scales. This metabolic transition is essential for maintaining the skin’s structural integrity and its ability to withstand constant friction and environmental exposure.
- Stem Cell Activity: Basal cells divide asymmetrically, producing one daughter cell that remains a stem cell and another that begins its ascent through the layers.
- Intercellular Communication: Gap junctions and desmosomes facilitate communication and mechanical strength throughout the spinosum and granulosum.
- Terminal Differentiation: The final stages of cell death are tightly controlled to ensure the surface barrier remains intact while allowing for the removal of old tissue.
Specialized Cells Residing in the Epidermis
While keratinocytes form the structural backbone of the epidermis, other specialized cells play vital roles in protection and sensation. Melanocytes, located in the stratum basale, produce melanin, which is packaged into melanosomes and transferred to nearby keratinocytes to protect their nuclei from UV radiation. Langerhans cells, found primarily in the stratum spinosum, act as the skin’s first-line immune defense by capturing antigens and presenting them to T-lymphocytes. Additionally, Merkel cells function as mechanoreceptors for light touch, closely associating with nerve endings at the epidermal-dermal junction.
The synergy between these cell types allows the skin to function not just as a passive wall, but as an active sensing and immune organ. For instance, the skin’s pigmentary response to sunlight is a complex interaction involving chemical signaling between keratinocytes and melanocytes. Similarly, the rapid response of Langerhans cells to topical irritants or pathogens is a crucial component of the body’s inflammatory and immune pathways.
Histological Variations: Thick Skin vs. Thin Skin
The appearance of the epidermis varies significantly depending on its location on the body. Thick skin, found on the palms and soles, is characterized by a very thick stratum corneum and the presence of a distinct stratum lucidum. This variation is an evolutionary adaptation to areas subject to high mechanical stress. In contrast, thin skin covers the majority of the body; it lacks a stratum lucidum and has a much thinner stratum corneum. Thin skin often contains hair follicles and sebaceous glands, which are notably absent in thick skin regions.
From a histological perspective, these differences are important for pathologists when examining skin biopsies. The relative thickness of the granulosum and the presence or absence of specific appendages help in identifying the anatomical site of a specimen. Furthermore, variations in the papillary dermis below the basement membrane—such as the prominence of dermal papillae—correlate with the mechanical demands placed on the overlying epidermis, providing extra surface area for attachment and nutrient exchange.
Clinical Implications of Epidermal Integrity
Many common skin disorders arise from a disruption in the normal functioning of the epidermal layers. For example, psoriasis is a condition where the rate of cell division in the stratum basale is greatly accelerated, leading to an buildup of immature cells on the surface that haven’t had time to properly keratinize. Eczema, on the other hand, often involves a defect in the skin’s barrier function, specifically within the lipid matrix of the stratum granulosum, making the skin susceptible to irritants and infections. Understanding the microscopic architecture helps clinicians choose targeted treatments, such as topical corticosteroids to reduce inflammation or emollients to restore the lipid barrier.
Furthermore, the basement membrane between the stratum basale and the dermis is a critical site for blistering diseases. Autoimmune conditions like bullous pemphigoid involve the immune system attacking the proteins that anchor the epidermis to the dermis, leading to painful blisters. In the context of wound healing, the re-epithelialization process depends entirely on the migration of basal cells from the wound edges and hair follicles to cover the exposed dermis and restore homeostasis.
Conclusion and Diagnostic Significance
In summary, the epidermis is a highly specialized tissue composed of distinct layers, each with a unique role in protecting the human body. From the proliferative stratum basale to the protective stratum corneum, the coordinated maturation of keratinocytes ensures a resilient and waterproof exterior. Mastery of this anatomy is indispensable for any medical professional, as it informs the understanding of everything from basic wound care to complex oncological conditions like basal cell carcinoma or melanoma. By appreciating the intricate histological details of the skin’s layers, we can better understand how this remarkable organ maintains its function and responds to the challenges of the external world.


{kind=link}
![[1]](http://www.nku.edu/~dempseyd/skin%20layers.jpg){kind=link}
{kind=link}