The anatomy of a newborn skull is one of the most remarkable examples of biological engineering in the human body. At the moment of birth, the infant’s head is not a single, solid bone but rather a collection of separate plates held together by flexible connective tissue. This unique arrangement serves a dual purpose: first, it allows the skull to ‘mold’ or compress slightly to pass through the mother’s birth canal; second, it provides the necessary space for the brain to expand rapidly during the first few years of life. For clinicians and parents alike, the ‘soft spots’ or fontanelles are essential indicators of health, providing a window into the internal environment of the developing cranium. By viewing the skull from a superior perspective, we can appreciate the precise geometry of these bones and sutures as they orchestrate a delicate balance between protection and growth.
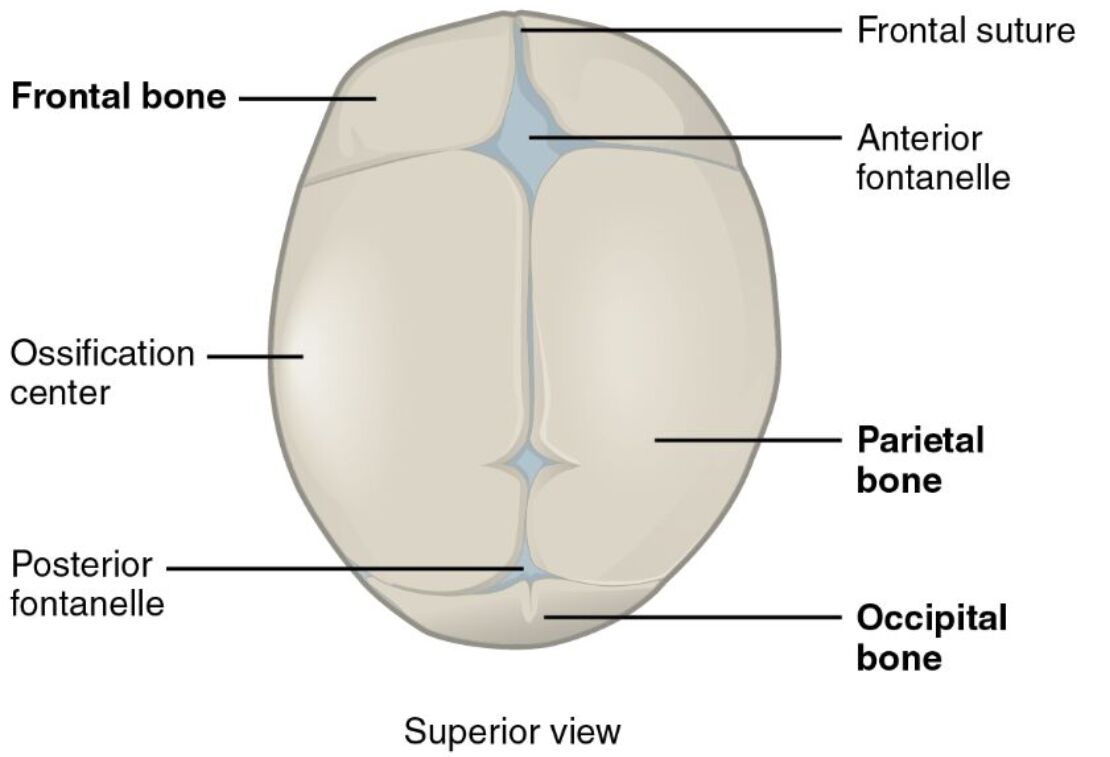
Frontal suture: This vertical line separates the two frontal bone plates in the infant, allowing the forehead to widen as the brain expands. It typically fuses by the second year of life, though a residual trace known as the metopic suture may persist in some adults.
Frontal bone: At birth, this structure exists as two distinct plates that eventually fuse into the single forehead bone. This separation is vital for the molding process during birth, where the plates can slightly overlap to facilitate passage through the birth canal.
Anterior fontanelle: Frequently referred to as the main soft spot, this diamond-shaped region is the junction where the frontal and parietal bones meet. It provides a reliable anatomical landmark for pediatricians to monitor hydration levels and intracranial pressure.
Ossification center: These are the initial sites where bone mineral begins to replace the flexible connective tissue of the fetal skull. As these centers grow, they radiate outward toward the sutures, gradually hardening the protective vault surrounding the brain.
Parietal bone: These two large bones form the upper and lateral sections of the skull vault. They are connected at the midline by the sagittal suture and play a significant role in protecting the parietal lobes of the brain.
Posterior fontanelle: This triangular-shaped gap is located at the back of the head where the parietal bones meet the occipital bone. It usually closes much earlier than its anterior counterpart, typically within the first few months after birth.
Occipital bone: Positioned at the base and back of the cranium, this bone protects the cerebellum and primary visual processing areas. In infants, it is relatively flexible and separated from the parietal bones by the posterior fontanelle.
The Biological Necessity of Fontanelles and Sutures
The human brain is an incredibly demanding organ, tripling in size during the first two years of life. To accommodate this explosive development, the newborn skull is equipped with fontanelles, which act as expansion joints. These membrane-covered gaps allow the brain to expand without being restricted by a rigid bone structure. If the skull were a solid cage at birth, the increasing pressure from brain growth would lead to severe neurological damage. Instead, the sutures—the flexible fibrous joints between the bones—stay open, allowing the skull to grow in direct proportion to the volume of the brain. This adaptive mechanism is a testament to the evolutionary tradeoff between the large human brain and the narrow pelvic dimensions required for upright walking.
Beyond growth, these spaces are critical for the mechanical challenges of delivery. The phenomenon of molding occurs when the parietal and frontal bones shift and overlap under the pressure of the birth canal. This temporary deformation often gives newborns a slightly conical or elongated head shape immediately after birth, which usually resolves within a few days. Without this flexibility, the risk of maternal and infant birth trauma would be significantly higher. Thus, the open sutures are not a sign of incompleteness but a highly functional state of transition.
Intramembranous Ossification: The Hardening Process
Unlike the long bones of the arms and legs, which develop from a cartilage template, the bones of the skull vault undergo a process called intramembranous ossification. In this pathway, bone is formed directly within a layer of mesenchymal or connective tissue. The ossification centers identified in the diagram are the starting points of this hardening. From these focal points, specialized cells called osteoblasts lay down mineralized matrix in a radial fashion. This explains why infant skull bones often feel thinner and more flexible at their edges near the fontanelles compared to the more central, hardened areas.
The timeline of this ossification is predictable and serves as a developmental milestone for healthcare providers. The posterior fontanelle typically closes by 2 to 3 months of age, as the parietal and occipital bones meet. The larger anterior fontanelle takes significantly longer, usually closing between 12 and 24 months. Monitoring the rate at which these spots close is a standard part of pediatric well-visits, as both premature and delayed closure can signify underlying health issues that require medical intervention.
Clinical Significance: The Fontanelle as a Health Window
Because the anterior fontanelle is a membrane-covered opening, it reacts to the pressure within the infant’s body. Pediatricians often palpate this area to assess a child’s clinical status. For example, a sunken fontanelle is a classic sign of severe dehydration, indicating that the overall fluid volume in the body is low. Conversely, a bulging fontanelle when the infant is at rest can be an indicator of increased intracranial pressure, possibly caused by meningitis, hydrocephalus, or trauma. This non-invasive ‘pressure gauge’ is an invaluable tool in early diagnostics.
Furthermore, the fontanelles provide an acoustic window for medical imaging. Because bone blocks ultrasound waves, the fontanelle allows doctors to use cranial ultrasound to view the brain’s internal structures, such as the ventricles and vascular supply, without the need for sedation or ionizing radiation from a CT scan. This makes the newborn period a unique time where high-quality brain imaging is easily accessible and safe, allowing for the early detection of hemorrhages or structural abnormalities that might not be visible from the outside.
Congenital Abnormalities and Skull Growth
When the delicate timing of skull growth goes awry, it can lead to conditions such as craniosynostosis. This occurs when one or more of the sutures fuse prematurely. Because the brain continues to grow, it is forced to expand in the directions where the sutures remain open, leading to an abnormally shaped head and potentially high pressure on the brain. For instance, if the sagittal suture (between the parietal bones) fuses early, the head becomes long and narrow. These conditions are often treated with reconstructive surgery to reopen the gaps and allow for normal brain development.
Other conditions, such as microcephaly or macrocephaly, may be suspected if the head circumference is significantly outside the normal range. In these cases, the fontanelles might close too early because the brain isn’t growing (microcephaly) or stay open much longer than usual (macrocephaly/hydrocephalus). By tracking head circumference alongside the status of the fontanelles and sutures, clinicians can differentiate between normal variations and pathological growth patterns, ensuring that every child receives the necessary support during these formative years.
Conclusion
The superior view of the newborn skull reveals a dynamic and adaptive structure that is perfectly suited for the journey from the womb to early childhood. The intricate interplay between the frontal, parietal, and occipital bones, governed by the flexible sutures and fontanelles, ensures that the infant is protected during birth while remaining capable of rapid growth. Understanding the milestones of ossification and the clinical signs associated with the soft spots allows for better monitoring of infant health and development. While it may seem fragile, the newborn skull is a robust and sophisticated anatomical system that serves as the foundation for a lifetime of neurological function. Recognizing the normal anatomical landscape is essential for identifying the rare deviations that require care, making the study of the neonatal cranium a cornerstone of pediatric medicine.


{kind=link}