This article provides a detailed anatomical and physiological overview of the penis, utilizing the provided diagrams to illustrate its structure in both flaccid and erect states. Understanding the intricate arrangement of erectile tissues, vasculature, and innervation is crucial for comprehending male sexual function and the mechanisms underlying erection. We will explore the key components of the penile anatomy and the hemodynamic changes that facilitate penile tumescence, offering insights into this vital aspect of reproductive health.
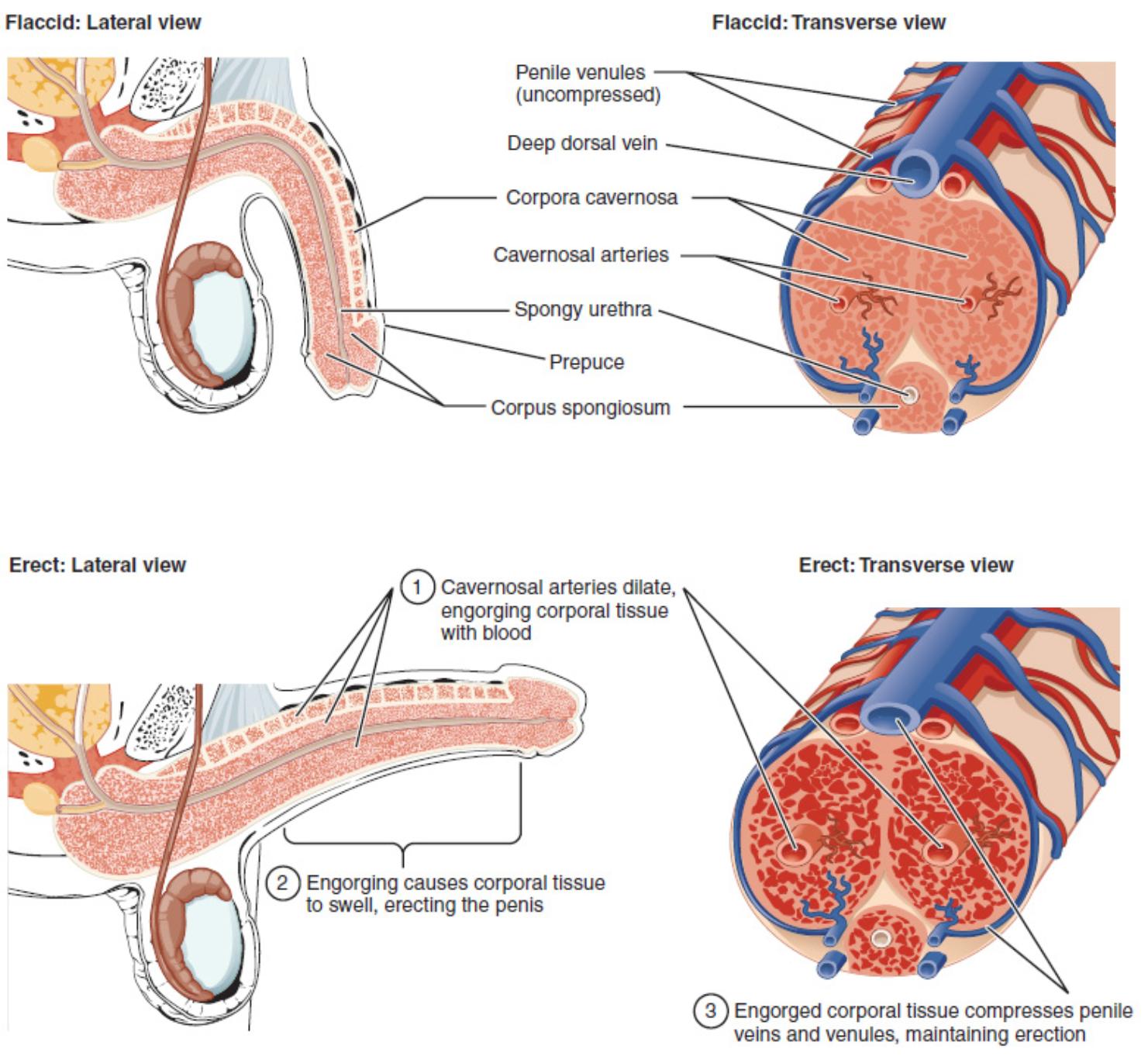
Diagram Labels and Explanations:
Penile venules (uncompressed): These are small veins within the penis that drain blood from the erectile tissues in the flaccid state. When uncompressed, they allow for a continuous outflow of blood, maintaining detumescence.
Deep dorsal vein: A major vein located on the dorsal aspect of the penis, lying deep to the deep fascia. It collects blood from the corpora cavernosa and drains into the prostatic venous plexus.
Corpora cavernosa: These are two columns of erectile tissue located dorsally within the shaft of the penis. They are composed of a spongy network of vascular spaces that fill with blood during erection, providing rigidity.
Cavernosal arteries: Also known as deep arteries of the penis, these arteries run longitudinally within the center of each corpus cavernosum. Their dilation is the primary event initiating erection, as they supply blood to the sinusoidal spaces.
Spongy urethra: This is the portion of the urethra that passes through the corpus spongiosum, extending from the bulb of the penis to the external urethral orifice. It serves as the conduit for both urine and semen.
Prepuce: Also known as the foreskin, this is a retractable fold of skin that covers the glans penis. Its presence or absence is determined by circumcision.
Corpus spongiosum: This is a single column of erectile tissue located ventrally, surrounding the spongy urethra. It expands distally to form the glans penis and proximally to form the bulb of the penis, remaining relatively pliable during erection to protect the urethra.
Cavernosal arteries dilate, engorging corporal tissue with blood (1): This describes the initial physiological event of an erection, where neural signals cause relaxation of smooth muscle in the cavernosal arteries, leading to increased blood flow into the corpora cavernosa and corpus spongiosum. This rapid influx of arterial blood is the primary driver of tumescence.
Engorging causes corporal tissue to swell, erecting the penis (2): As blood rapidly fills the sinusoidal spaces within the corpora cavernosa and corpus spongiosum, these erectile tissues expand significantly. This swelling causes the penis to enlarge and become rigid, transitioning from a flaccid to an erect state.
Engorged corporal tissue compresses penile veins and venules, maintaining erection (3): The expansion of the corpora cavernosa against the tunica albuginea, and the compression of the subtunical venules, restricts venous outflow. This veno-occlusion mechanism is crucial for trapping blood within the erectile tissues, thereby maintaining the rigidity of the erection.
Penile Anatomy and the Mechanism of Erection
The human penis is a marvel of biological engineering, primarily composed of three columns of specialized erectile tissue, as clearly illustrated in the provided diagrams. These structures—two dorsally positioned corpora cavernosa and a single ventral corpus spongiosum—are encased within a tough fibrous sheath called the tunica albuginea, and together they form the core of penile function. Understanding the interplay of these tissues and their vascular supply is essential for grasping the mechanics of erection.
In the flaccid state, the penis is characterized by limited blood flow into the erectile tissues and continuous venous drainage. The cavernosal arteries are constricted, allowing only a small amount of blood to enter the sinusoidal spaces within the corpora cavernosa. Simultaneously, the penile venules remain uncompressed, facilitating a free outflow of blood. This balance maintains the penis in its resting, non-erect state. The spongy urethra, embedded within the corpus spongiosum, remains unobstructed, allowing for urine passage.
The initiation of an erection is a neurovascular event triggered by sexual stimulation. This leads to the release of neurotransmitters, primarily nitric oxide, which causes the smooth muscles in the walls of the cavernosal arteries to relax.
- Arterial Dilation and Blood Inflow: The relaxation of these muscles results in a dramatic dilation of the cavernosal arteries, leading to a rapid and substantial increase in blood flow into the sinusoidal spaces of the corpora cavernosa and corpus spongiosum. This is depicted as step (1) in the erect view.
- Tissue Engorgement and Swelling: As these spaces quickly fill with arterial blood, the corporal tissue engorges and swells significantly, causing the penis to enlarge and become rigid, as shown in step (2).
- Veno-occlusion and Erection Maintenance: The expanding corpora cavernosa press against the inelastic tunica albuginea, which in turn compresses the subtunical venules against the outer sheath. This compression effectively reduces venous outflow (veno-occlusion), trapping blood within the erectile tissues and maintaining the erection (step 3). The corpus spongiosum, which surrounds the urethra, also engorges but to a lesser extent, ensuring the urethra remains patent for ejaculation.
Conclusion
The cross-sectional anatomy of the penis, in both its flaccid and erect states, reveals a sophisticated interplay of vascular and erectile tissues. The transition from flaccidity to erection is a finely tuned hemodynamic process involving arterial dilation, rapid blood inflow, and subsequent veno-occlusion, all orchestrated by neural and biochemical signals. This detailed understanding of penile structure and the physiology of erection is foundational to the fields of urology and reproductive medicine, providing insights into normal sexual function and the basis for various erectile dysfunctions.


{kind=link}