Radiographic interpretation is a foundational skill in pulmonary medicine, serving as the first line of defense in identifying life-threatening respiratory conditions. Among the various findings visible on a chest X-ray, the presence of a cavity represents a significant structural change that often signals severe underlying pathology. A cavity is defined as a gas-filled space within a zone of pulmonary consolidation or a mass, usually formed by the expulsion of a necrotic part of the lesion through the bronchial tree. This radiological hallmark is not merely an incidental finding but a critical diagnostic clue that narrows down a wide range of possibilities, from infectious diseases like tuberculosis to malignant growths. Understanding the nuances of cavitary presentations is essential for clinicians to initiate timely interventions and prevent further tissue destruction. By analyzing the wall thickness, the location, and the surrounding lung parenchyma, radiologists and physicians can piece together a diagnostic puzzle that directs the patient toward the most effective treatment pathway.
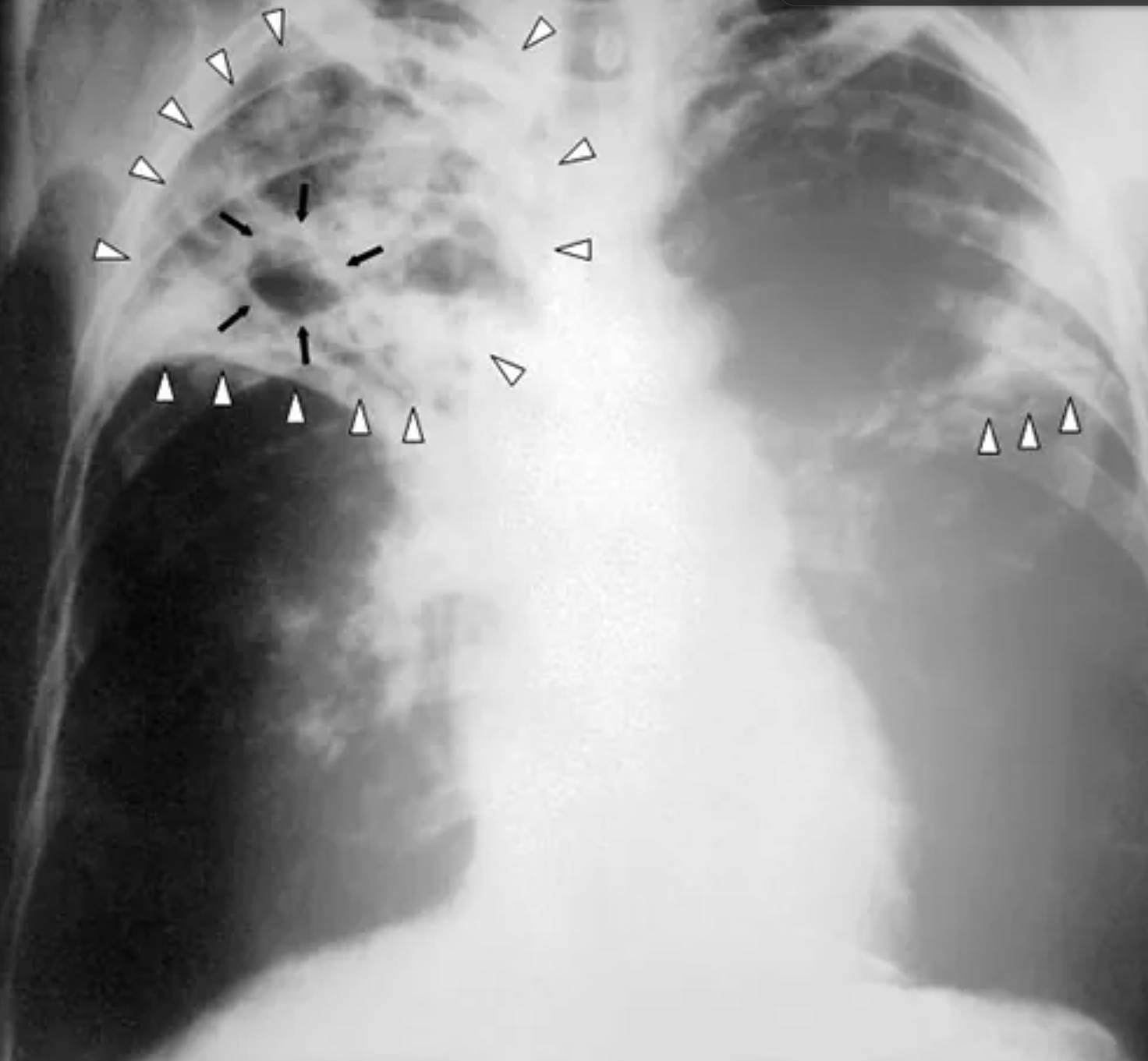
Black Arrows: These arrows highlight a well-defined pulmonary cavity, appearing as a radiolucent, air-filled void within an area of high density. This finding indicates that a portion of the lung tissue has undergone liquefactive necrosis and has been evacuated, usually through a communicating bronchus.
White Hollow Arrowheads: These markers delineate extensive patchy opacities and areas of consolidation scattered throughout both the right and left upper lung fields. These findings represent inflammatory exudate or solid material filling the alveoli, which is highly characteristic of an active and spreading infectious process.
White Solid Arrowheads: These indicators point to the inferior boundary of the primary consolidated mass in the right lung. They help the clinician visualize the total volume of lung tissue affected by the inflammatory response and the subsequent density changes on the radiograph.
The Pathophysiology of Lung Cavity Formation
The development of a pulmonary cavity is a multi-step biological process that begins with localized tissue injury. When a pathogen or a malignant process invades the lung parenchyma, it triggers an intense inflammatory response. In many cases, this leads to necrosis, where the cells and structural proteins of the lung essentially die. If the dead tissue undergoes liquefaction—turning into a semi-liquid state—it can be coughed up and cleared through the bronchial tubes. Once the necrotic material is removed, a hole or “cavity” remains, filled only with air. This process is most famously seen in secondary tuberculosis, where the body’s immune response to the bacteria is so vigorous that it destroys its own tissue to contain the spread.
The radiological appearance of these cavities provides vital clues. For instance, a cavity with a very thin wall (less than 1mm) is often benign, such as a cyst or a bulla. However, cavities with thick, irregular walls are much more concerning and often point toward bacterial abscesses or squamous cell carcinoma. Furthermore, the presence of an “air-fluid level” within a cavity—where the bottom half looks white and the top half looks dark—suggests that there is still liquid pus or blood trapped inside that has not yet been fully drained. The physician must monitor these changes closely, as a growing cavity can lead to complications like hemoptysis (coughing up blood) if it erodes into an adjacent blood vessel.
Differential Diagnosis of Cavitary Lesions
The presence of lung cavity formation on a chest X-ray triggers a comprehensive diagnostic search. Medical students often use the mnemonic “CAVITY” to remember the primary causes: C (Cancer, particularly squamous cell carcinoma), A (Autoimmune diseases like granulomatosis with polyangiitis), V (Vascular issues like pulmonary embolism leading to infarction), I (Infection), T (Trauma), and Y (Youth/Congenital issues like bronchogenic cysts). Among these, infection remains the most common culprit globally. Bacterial infections like Staphylococcus aureus or Klebsiella pneumoniae are known for causing rapidly developing cavities, often referred to as lung abscesses.
However, when a patient presents with chronic symptoms such as weight loss, night sweats, and a persistent cough alongside upper-lobe cavitary lesions, the primary suspicion is tuberculosis. In the reactivation phase of this disease, the bacteria thrive in the oxygen-rich environment of the lung’s upper segments. Fungal infections, such as aspergillosis, can also create cavities or colonize existing ones, forming what is known as a “fungus ball” or aspergilloma. Because the treatment for a bacterial abscess is vastly different from the treatment for cancer or tuberculosis, the differential diagnosis must be meticulously narrowed down through sputum cultures, blood tests, and often more advanced imaging like Computed Tomography (CT).
Diagnostic Approach and Imaging Modalities
While the standard posteroanterior (PA) chest X-ray seen in the image is the traditional starting point, it has limitations in terms of sensitivity and detail. A PA radiograph can sometimes miss small cavities hidden behind the heart or the diaphragm. If a clinician suspects a cavity but the X-ray is inconclusive, a CT scan of the chest is the gold standard. CT imaging provides a three-dimensional view, allowing for much better assessment of the cavity’s wall characteristics, the presence of internal debris, and the exact relationship between the lesion and nearby vascular structures. It can also detect “satellite lesions,” which are smaller spots of infection or cancer nearby that might be invisible on a standard X-ray.
- Sputum Analysis: Essential for identifying bacterial, mycobacterial (TB), or fungal pathogens.
- Bronchoscopy: A procedure where a camera is inserted into the airways to take direct tissue samples or washings from the affected area.
- CT-Guided Biopsy: Necessary if malignancy is suspected and the lesion is in a location that can be safely reached with a needle.
- Serology: Blood tests to look for autoimmune markers or specific fungal antigens.
Integrating these findings with the patient’s clinical history—such as recent travel, smoking history, or immune status—is the only way to reach a definitive diagnosis. For example, a cavity in an immunocompromised patient is managed with much higher urgency than one in a healthy individual, as the risk of rapid progression and systemic spread is significantly higher.
Clinical Management and Treatment Pathways
The management of a lung cavity is entirely dependent on its root cause. If the diagnosis is a bacterial lung abscess, long-term intravenous antibiotics are typically required, often for several weeks, until the cavity begins to close. In cases of tuberculosis, a strict multi-drug regimen lasting at least six months is necessary to ensure the bacteria are completely eradicated and to prevent the development of drug-resistant strains. If the cavity is caused by a fungal infection, specialized antifungal medications are used, though surgical removal of the affected lung lobe (lobectomy) might be required if the fungal mass causes life-threatening bleeding.
When the cavity is a result of malignancy, the focus shifts to staging the cancer and determining if surgery, radiation, or chemotherapy is the best course of action. Regardless of the cause, follow-up imaging is a mandatory part of the process. Physicians must see the cavity shrinking over time to confirm that the treatment is working. A cavity that remains “non-healing” or continues to expand despite therapy is a major red flag that requires a re-evaluation of the diagnosis or a switch to more aggressive treatment strategies. Through careful radiological monitoring and multidisciplinary care, many patients with cavitary lung disease can achieve full recovery, though some permanent scarring of the lung tissue is common.
Conclusion
The identification of a lung cavity on a radiograph is a pivotal moment in patient care, demanding a thorough and systematic investigation. As we have seen, these air-filled voids are the visible scars of complex pathological processes, ranging from the aggressive tissue destruction of tuberculosis to the silent growth of malignant tumors. By combining the visual data from chest X-rays and CT scans with clinical expertise, healthcare providers can navigate the intricate differential diagnosis and tailor treatments to the specific needs of the patient. While the sight of a cavity in the lung can be alarming, modern diagnostics and therapeutics offer robust pathways for management and healing. Continued vigilance and a deep understanding of pulmonary anatomy remain our best tools in the ongoing fight against respiratory disease.


{kind=link}