The medial view of the foot is perhaps the most clinically significant perspective for understanding the biomechanics of human ambulation. It provides a clear visualization of the medial longitudinal arch—the highest and most important of the three foot arches—which serves as a dynamic shock absorber and a rigid lever during the gait cycle. This view allows clinicians to evaluate the alignment of the tarsal bones, the integrity of the midfoot joints, and the structural relationships between the hindfoot and the forefoot, all of which are critical for diagnosing conditions ranging from flatfoot deformities to traumatic fractures.
Label-by-Label Explanation
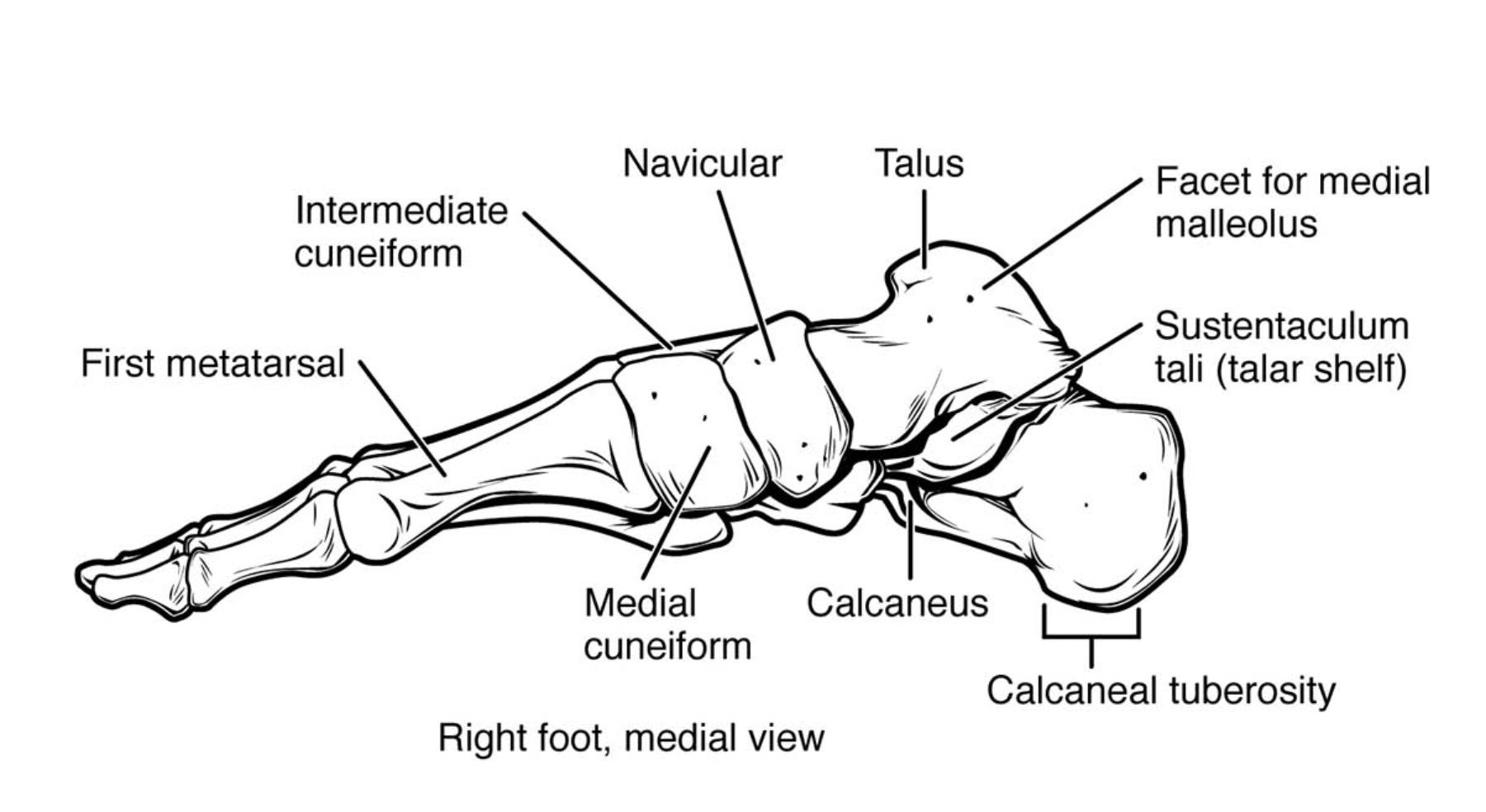
Intermediate cuneiform
The intermediate cuneiform is the smallest of the three cuneiform bones, located between the medial and lateral cuneiforms. It articulates distally with the second metatarsal, contributing to the stability of the midfoot mortise. Clinically, its dorsal surface is a palpable landmark used to localize midfoot pain and assess tarsometatarsal joint integrity.
Navicular
The navicular is a boat-shaped tarsal bone situated between the head of the talus and the three cuneiform bones. It serves as the primary insertion point for the tibialis posterior tendon, which is the main dynamic stabilizer of the medial longitudinal arch. Dysfunction or stress fractures in the navicular can lead to significant arch collapse and chronic medial foot pain.
Talus
The talus is the second largest tarsal bone and is unique because it lacks any muscular attachments, receiving its entire blood supply through ligamentous attachments and articular capsules. It functions as the primary weight-bearing link between the leg and the foot, articulating with the tibia and fibula superiorly and the calcaneus inferiorly. Its role is essential for transmitting vertical forces from the body into the longitudinal arches of the foot.
Facet for medial malleolus
This articular surface on the medial aspect of the talar body articulates with the medial malleolus of the tibia. This joint allows for the hinge-like motion of the ankle, specifically dorsiflexion and plantarflexion. Integrity of this facet for medial malleolus is crucial for joint stability and preventing chronic ankle arthrosis following traumatic injury.
Sustentaculum tali (talar shelf)
The sustentaculum tali is a horizontal, shelf-like projection from the medial surface of the calcaneus that supports the neck of the talus. It forms the floor of the tarsal tunnel, with the flexor hallucis longus tendon passing directly beneath it. Fractures of this structure can compromise the subtalar joint and lead to impingement of the medial neurovascular bundle.
Calcaneus
The calcaneus, or heel bone, is the largest and strongest bone in the human foot, designed to sustain the impact of heel strike during gait. It provides the base for the posterior portion of the longitudinal arches and acts as a massive lever for the triceps surae muscles. Its dense cancellous bone structure is often analyzed on X-rays to assess bone mineral density or detect complex intra-articular fractures.
Calcaneal tuberosity
The calcaneal tuberosity is the large, roughened posterior projection of the calcaneus where the Achilles (calcaneal) tendon inserts. It serves as the primary attachment point for the plantar fascia and the intrinsic muscles of the sole. Clinically, it is a frequent site of enthesopathy, such as Achilles tendonitis, Haglund’s deformity, or plantar fasciitis.
Medial cuneiform
The medial cuneiform is the largest of the cuneiform bones and is situated at the medial border of the midfoot. It articulates distally with the first metatarsal, forming the first tarsometatarsal joint, which is a key component of the ‘first ray’ of the foot. Its orientation is vital for maintaining the height of the medial longitudinal arch and enabling efficient toe-off during propulsion.
First metatarsal
The first metatarsal is the shortest, thickest, and strongest of the metatarsal bones, bearing the most significant load during the terminal stance phase of walking. It provides the skeletal framework for the hallux (great toe) and articulates with the sesamoid bones on its plantar surface. Deviations in its alignment relative to the medial cuneiform often lead to hallux valgus (bunions).
Anatomical Overview
The medial view effectively demonstrates the ‘medial column’ of the foot, which is the primary structure involved in shock absorption. This column consists of the talus, navicular, the three cuneiforms, and the medial three metatarsals. Structurally, the medial column is more mobile and resilient than the lateral column, allowing the foot to adapt to surface irregularities while maintaining stability.
The intersection where the talar head meets the navicular (the talonavicular joint) is often referred to as the ‘keystone’ of the medial longitudinal arch. Above this, the ankle joint is formed by the facet for medial malleolus articulating with the tibia. Below, the subtalar joint between the talus and calcaneus allows for inversion and eversion movements, which are essential for navigating uneven terrain.
Functional Significance
The medial longitudinal arch is a complex functional unit that relies on both passive and active stabilizers. Passive stability is provided by the interlocking shapes of the tarsal bones, particularly the wedge-shaped cuneiforms and the boat-shaped navicular. The most important passive stabilizer is the plantar calcaneonavicular (spring) ligament, which spans the gap between the sustentaculum tali and the navicular, supporting the head of the talus.
Active stability is provided by muscles such as the tibialis posterior, whose tendon inserts on the navicular. During the stance phase of gait, these structures allow the arch to slightly flatten to absorb energy and then quickly recoil to transform the foot into a rigid lever for propulsion. The first metatarsal plays a final crucial role in this process by serving as the primary anchor point for toe-off.
Clinical Relevance
In clinical practice, the medial view is indispensable for evaluating pes planus (flatfoot) and pes cavus (high arches). On weight-bearing lateral radiographs, which correspond to this medial anatomical view, clinicians measure Meary’s angle—the angle between the long axis of the talus and the first metatarsal. A break in this collinear relationship indicates arch collapse, often due to posterior tibial tendon dysfunction.
Traumatic injuries also frequently involve the medial structures. Fractures of the sustentaculum tali are rare but significant, as they can lead to subtalar joint instability and medial tarsal tunnel syndrome. Furthermore, the calcaneal tuberosity is a common site for stress fractures in long-distance runners and is the focus of treatment for chronic plantar fasciitis. Understanding the exact insertion of the Achilles tendon here is vital for surgical procedures involving Haglund’s deformity excision.
Diagnostic or Educational Importance
Mastering the medial anatomy of the foot is essential for performing accurate physical examinations. Palpating the navicular tubercle or the medial cuneiform allows a practitioner to differentiate between midfoot sprains, tendinopathies, and stress fractures. In imaging studies, understanding the relationship between the talar body and the calcaneus helps in identifying subtalar coalitions, which are a common cause of rigid flatfoot in adolescents.
For medical students, this view bridges the gap between basic osteology and functional biomechanics. By learning how the talus distributes weight through the navicular to the forefoot, students can better appreciate the systemic effects of foot malalignment on the knee, hip, and lower back. Educational focus should remain on the three-dimensional interlocking nature of these bones rather than just their individual names.
In summary, the bones of the medial foot form the structural backbone of human locomotion. From the weight-bearing capacity of the calcaneus to the propulsive power of the first metatarsal, every structure in this medial view serves a specific mechanical purpose. Clinicians must maintain a high level of anatomical proficiency in this area to effectively treat the wide variety of gait-related and traumatic disorders that affect the lower extremity.
Medical Learning Tips
- The sustentaculum tali acts as a pulley for the flexor hallucis longus tendon, which passes directly beneath it.
- The navicular bone is often called the 'keystone' of the medial arch because its displacement causes immediate arch collapse.
- The first metatarsal bears approximately double the weight of any other metatarsal during the push-off phase of gait.


{kind=link}