Periodontal Anatomy: Understanding the Structural Components of the Tooth-Supporting Apparatus
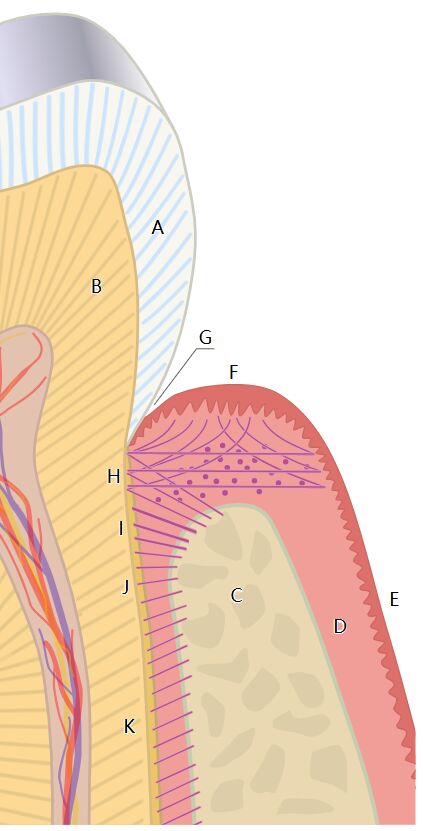
The periodontal apparatus represents a complex biological system that provides crucial support, nutrition, and sensory functions to the teeth. This detailed anatomical illustration depicts the key structures that comprise the periodontium, including the gingival tissue, periodontal ligament fibers, cementum, and alveolar bone. Together, these specialized tissues form a functional unit that anchors teeth within the jaw while allowing for minute movements during mastication and absorbing occlusal forces. The tooth is attached to the surrounding gingival tissue and alveolar bone (C) by fibrous attachments. The gingival fibers (H) run from the cementum (B) into the gingiva immediately apical to the junctional epithelial attachment, while the periodontal ligament fibers (I), (J), and (K) run from the cementum into the adjacent cortex of the alveolar bone. Understanding the normal anatomy and histology of these tissues is essential for dental professionals to accurately diagnose and treat periodontal conditions, perform surgical procedures, and implement effective preventive strategies to maintain periodontal health.
Labeled Structures in the Periodontal Anatomy Illustration
Label A: Enamel. This highly mineralized outer layer of the tooth crown is composed of approximately 96% hydroxyapatite crystals, making it the hardest substance in the human body. Enamel provides protection for the underlying dentin and pulp while withstanding the significant forces of mastication.
Label B: Dentin. This mineralized tissue forms the bulk of the tooth structure and is composed of approximately 70% inorganic material, 20% organic material (primarily type I collagen), and 10% water. Dentin contains microscopic tubules that radiate from the pulp chamber to the dentinoenamel or dentinocemental junction, contributing to tooth sensitivity when exposed.
Label C: Alveolar bone. This specialized portion of the maxillary and mandibular bones forms the sockets (alveoli) that house the teeth. Alveolar bone consists of an outer cortical plate, inner cancellous bone, and the cribriform plate (lamina dura) that lines the tooth socket and provides attachment for principal periodontal ligament fibers.
Label D: Cancellous bone. Also called trabecular or spongy bone, this less dense inner portion of the alveolar process consists of a network of bone trabeculae with intervening marrow spaces. Cancellous bone provides nutrients and contributes to the overall strength of the alveolar process while allowing for remodeling in response to functional demands.
Label E: Cortical bone. This dense, compact outer layer of the alveolar process provides structural integrity and resistance to occlusal forces. The thickness of cortical bone varies by location, with thicker plates typically found on the facial aspect of anterior teeth and lingual aspect of posterior teeth.
Label F: Free gingiva. This unattached portion of the gingiva extends from the gingival margin to the base of the gingival sulcus and is not directly connected to the tooth surface. The free gingiva forms a collar around the tooth and is separated from the attached gingiva by the free gingival groove.
Label G: Gingival sulcus. This shallow groove or space between the free gingiva and the tooth surface has a depth of 1-3 mm in healthy conditions. The gingival sulcus is lined by sulcular epithelium and contains gingival crevicular fluid, which provides immunological protection and diagnostic information about periodontal health.
Label H: Junctional epithelium. This specialized epithelium forms the epithelial attachment between the gingiva and the tooth surface, extending from the base of the gingival sulcus to the cementoenamel junction. The junctional epithelium attaches to the tooth via hemidesmosomes and a basal lamina, creating a crucial biological seal that protects deeper periodontal tissues.
Label I: Gingival fibers. These collagen fiber bundles within the gingival connective tissue help maintain the integrity and adaptation of the gingiva to the tooth. Gingival fibers include dentogingival, dentoperiosteal, circular, semicircular, and transseptal groups, each serving specific functional roles in gingival stability.
Label J: Periodontal ligament. This specialized connective tissue occupies the space between the tooth root and the alveolar bone socket, ranging from 0.15-0.38 mm in width. The periodontal ligament contains collagen fibers, blood vessels, nerves, and cellular elements that contribute to tooth support, sensory function, and nutritive supply.
Label K: Principal fibers of the periodontal ligament. These densely arranged collagen fiber bundles connect the cementum to the alveolar bone proper and are organized into distinct groups (alveolar crest, horizontal, oblique, apical, and interradicular) based on their orientation and attachment points. The principal fibers provide primary support for the tooth while allowing controlled movement during function.
Understanding the Periodontal Attachment Apparatus
The Dynamic Nature of Periodontal Tissues
Periodontal tissues demonstrate remarkable adaptability to functional demands and environmental changes. This dynamic nature is essential for maintaining the structural integrity of the tooth-supporting apparatus.
- The periodontal ligament undergoes continuous remodeling with an estimated turnover time of 5-7 days for collagen fibers, making it the most rapidly remodeling connective tissue in the body.
- This rapid turnover allows for adaptation to orthodontic forces, occlusal changes, and healing following injury or surgical intervention.
The balanced relationship between formation and resorption processes in periodontal tissues maintains structural homeostasis. Disruption of this balance can lead to pathological conditions.
- Osteoblasts, osteoclasts, fibroblasts, and cementoblasts work in coordinated fashion to maintain the structural integrity of the periodontium.
- Regulatory factors including cytokines, growth factors, and mechanical stimuli influence cellular activity and matrix remodeling in response to functional demands.
Cementum: The Connection Between Tooth and Periodontium
Cementum, though not specifically labeled in the illustration but referred to in the description as structure B, plays a critical role in anchoring the tooth to surrounding tissues. This mineralized tissue covers the anatomical root of the tooth.
- Primary acellular cementum covers the cervical third to half of the root and contains densely packed extrinsic (Sharpey’s) fibers that anchor the principal fibers of the periodontal ligament.
- Secondary cellular cementum occupies the apical portion of the root and contains both intrinsic fibers and entrapped cementocytes within lacunae, providing adaptive potential throughout life.
The cementum-periodontal ligament interface represents a critical functional junction in the attachment apparatus. This interface demonstrates remarkable resilience under normal functional conditions.
- Sharpey’s fibers penetrate approximately 30-50% into the cementum thickness, creating a strong mechanical interlock.
- Unlike bone, cementum does not undergo physiological resorption under normal conditions, contributing to the stability of the attachment apparatus.
Functional Organization of Periodontal Ligament Fibers
Principal Fiber Groups and Their Significance
The principal fibers of the periodontal ligament (labels I, J, and K) are arranged in specific orientations to resist various forces applied to the tooth. This architectural design optimizes mechanical support.
- Alveolar crest fibers extend obliquely from the cementum cervically to the alveolar crest, resisting extrusive forces and lateral movements.
- Horizontal fibers run perpendicular to the long axis of the tooth from cementum to alveolar bone, counteracting lateral and rotational forces.
The oblique fiber group constitutes approximately 60-70% of all principal fibers, making it the most significant component of the attachment apparatus. These fibers are particularly important in functional support.
- Oblique fibers extend from cementum coronally to alveolar bone apically, effectively converting axial occlusal forces into tension on the alveolar bone.
- This arrangement allows occlusal forces to stimulate bone formation rather than causing pressure-induced resorption, exemplifying the functional adaptation of the periodontium.
Gingival Fiber Apparatus
The gingival fiber system (label H) provides additional support and maintains the relationship between the gingival tissues and the tooth surface. This complex network includes several functionally distinct fiber groups.
- Dentogingival fibers extend from the cementum into the free and attached gingiva, maintaining the adaptation of the gingival margin to the tooth surface.
- Circular fibers run circumferentially around the tooth, reinforcing the free gingiva and contributing to its resistance against deformation during function.
Transseptal fibers connect adjacent teeth by extending horizontally from the cementum of one tooth to that of the neighboring tooth. These fibers have significant clinical implications.
- Transseptal fibers maintain proximal contact relationships between adjacent teeth and can contribute to the migration of teeth following extractions.
- These fibers remain intact even in periodontitis-affected sites and can be utilized in regenerative therapeutic approaches.
Vascular and Neural Components of the Periodontium
Microcirculation and Nutrient Supply
The periodontal tissues are richly vascularized, reflecting their high metabolic activity and defensive functions. This vascular network is crucial for tissue homeostasis.
- The periodontal ligament receives blood supply from three primary sources: apical vessels, penetrating vessels from the alveolar bone, and anastomosing vessels from the gingiva.
- This rich anastomotic network provides collateral circulation that supports healing following surgical procedures and protects against ischemic damage.
The gingival microcirculation has a distinctive arrangement that supports its specialized functions. The architectural organization of gingival vessels has important clinical implications.
- Capillary loops in the gingival connective tissue papillae lie close to the epithelium, facilitating the exchange of nutrients and defense components.
- The subepithelial plexus beneath the junctional epithelium represents an important pathway for inflammatory cells to enter the gingival sulcus during the immune response.
Neural Elements and Sensory Function
The periodontium contains a complex neural network that provides proprioceptive, nociceptive, and autonomic functions. These neural elements contribute to the sensory experience and reflex regulation of masticatory function.
- Periodontal mechanoreceptors detect tooth loads, positions, and movements, providing essential feedback for masticatory muscle activity and occlusal force control.
- The high density of sensory receptors allows detection of incredibly small interocclusal objects (as little as 20 microns), demonstrating the remarkable sensitivity of the system.
Autonomic innervation regulates vascular tone and influences inflammatory responses within periodontal tissues. This neural-immune interaction has significant implications for periodontal pathology.
- Sympathetic fibers primarily control vasoconstriction and can modulate immune cell function within the periodontium.
- Neuropeptides released from sensory nerve endings contribute to neurogenic inflammation and may play a role in periodontal disease progression.
Clinical Significance of Periodontal Anatomy
Implications for Periodontal Disease Progression
Understanding the structural organization of the periodontium provides insight into patterns of disease progression and tissue destruction. The architecture of periodontal tissues influences pathological processes.
- The junctional epithelium represents the first line of defense against bacterial invasion, with its relatively high permeability allowing immune surveillance but also creating potential vulnerability.
- The orientation of periodontal ligament fibers influences the pattern of bone destruction in periodontitis, with angular bone defects often developing in relation to the principal fiber arrangement.
The vascularity of periodontal tissues contributes to both protective and destructive aspects of the inflammatory response. This dual role highlights the complex nature of periodontal pathology.
- The rich blood supply facilitates rapid mobilization of immune defenses but also allows for widespread distribution of inflammatory mediators.
- Vascular changes, including increased permeability and angiogenesis, are early features of gingival inflammation that precede clinical signs of disease.
Considerations for Periodontal Therapy
Surgical and non-surgical periodontal therapies are designed based on understanding the anatomical structures depicted in this illustration. Preservation or regeneration of these structures is the ultimate goal of treatment.
- Scaling and root planing aims to remove bacterial biofilm and calculus from the root surface to allow reattachment of periodontal fibers and formation of a long junctional epithelium.
- Periodontal flap procedures must consider the blood supply to ensure adequate healing and maintenance of tissue viability following surgical manipulation.
Regenerative procedures attempt to reconstruct the original architecture of the periodontium following disease-induced destruction. These techniques are guided by principles of developmental biology.
- Guided tissue regeneration uses barrier membranes to exclude epithelial and gingival connective tissue cells, allowing periodontal ligament and bone cells to repopulate the wound area.
- Growth factors and tissue engineering approaches aim to stimulate cementum formation, periodontal ligament regeneration, and alveolar bone reconstruction in a coordinated sequence.
Conclusion
The complex architectural organization of periodontal tissues illustrated in this anatomical diagram demonstrates the sophisticated engineering of the tooth-supporting apparatus. Each component—from the mineralized tissues of dentin, cementum, and alveolar bone to the soft tissue elements of gingiva and periodontal ligament—contributes to the remarkable functional capacity of this system. The precise arrangement of collagen fiber bundles, vascular networks, and neural elements allows the periodontium to withstand significant mechanical forces while maintaining sensory function and defensive capabilities. For dental professionals, a thorough understanding of this anatomy is foundational to clinical practice, influencing everything from diagnostic interpretation to treatment planning and surgical technique. As research continues to uncover the molecular and cellular mechanisms underlying periodontal development, homeostasis, and regeneration, this anatomical knowledge becomes increasingly valuable in developing innovative therapeutic approaches to periodontal disease and reconstruction.
- Periodontal Attachment Apparatus: Comprehensive Guide to Gingival Fibers, Cementum, and Alveolar Bone
- Understanding the Periodontal Ligament Complex: Anatomical Structure and Clinical Significance
- Dental Supporting Tissues: Detailed Exploration of the Periodontium and Attachment Apparatus
- Periodontal Anatomy Explained: From Gingival Fibers to Alveolar Bone Architecture
- The Tooth-Supporting Structures: An In-depth Analysis of Periodontal Tissue Organization


{kind=link}