This comprehensive anatomical guide provides a detailed analysis of the medial view of the hip bone, also known as the coxal bone or os coxae. By examining the labeled structures such as the iliac fossa, auricular surface, and ischial spine, medical students and professionals can gain a deeper understanding of pelvic osteology and its functional significance in the human body, particularly regarding weight transmission and muscle attachment.
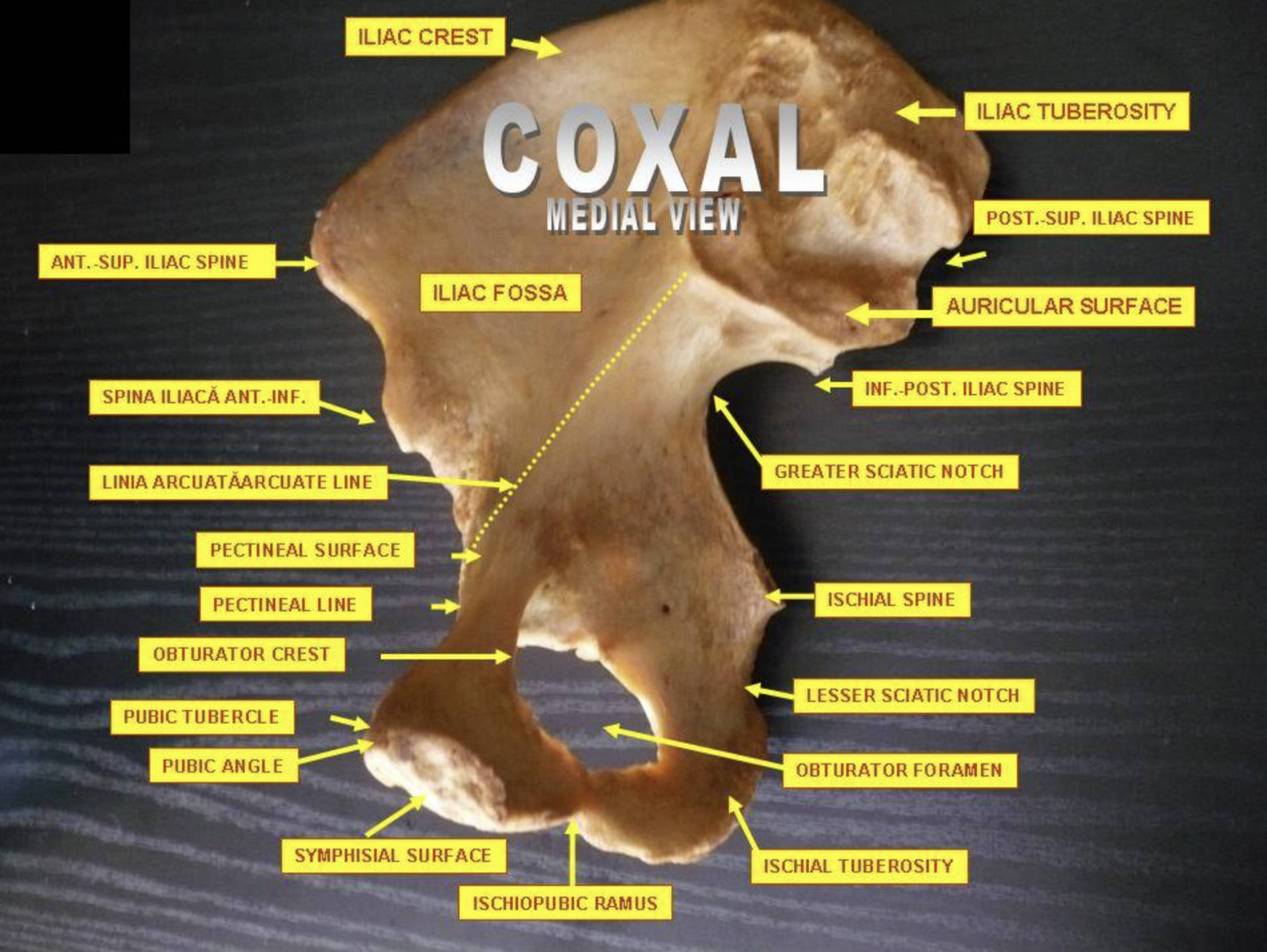
Iliac Crest: This is the prominent, arched superior border of the ilium, easily palpable on the sides of the waist. It serves as a crucial attachment site for abdominal muscles, such as the internal and external obliques, as well as the latissimus dorsi.
Iliac Tuberosity: Located posteriorly to the iliac fossa and superior to the auricular surface, this is a rough, elevated area of bone. It provides a strong attachment point for the posterior sacroiliac ligaments, which stabilize the connection between the hip and the spine.
Post.-Sup. Iliac Spine (Posterior Superior Iliac Spine): This landmark marks the posterior end of the iliac crest. While difficult to palpate due to tissue coverage, its position is often indicated by a visible skin dimple on the lower back at the level of the second sacral vertebra.
Auricular Surface: This ear-shaped articular surface is located on the medial aspect of the ilium. It is covered with fibrocartilage and articulates with the sacrum to form the sacroiliac joint, a critical weight-bearing joint.
Inf.-Post. Iliac Spine (Posterior Inferior Iliac Spine): Situated just below the auricular surface, this projection marks the superior border of the greater sciatic notch. It serves as an attachment point for the sacrotuberous ligament.
Greater Sciatic Notch: This deep indentation is located beneath the posterior inferior iliac spine. It is converted into the greater sciatic foramen by the sacrotuberous and sacrospinous ligaments, allowing the passage of the piriformis muscle and the sciatic nerve.
Ischial Spine: This is a triangular, pointed prominence located posterior to the acetabulum. It acts as a separator between the greater and lesser sciatic notches and serves as the attachment site for the sacrospinous ligament.
Lesser Sciatic Notch: Found directly below the ischial spine, this smaller indentation is smooth and shallow. It transmits the tendon of the obturator internus muscle and the nerve to the obturator internus out of the pelvis.
Obturator Foramen: This is the large opening created by the ischium and pubis bones, situated inferior to the acetabulum. In a living body, it is almost completely closed by the fibrous obturator membrane, leaving only a small canal for the passage of obturator vessels and nerves.
Ischial Tuberosity: Commonly referred to as the “sit bone,” this is a large, rough swelling at the inferior part of the ischium. It supports the body’s weight when sitting and provides the origin for the hamstring muscles.
Ischiopubic Ramus: This structure is formed by the fusion of the inferior ramus of the pubis and the ramus of the ischium. It forms the inferior boundary of the obturator foramen and serves as an attachment for muscles of the medial thigh.
Symphisial Surface: This oval-shaped, rough surface is located on the medial aspect of the body of the pubis. It articulates with the corresponding surface of the opposite hip bone via a fibrocartilaginous disc to form the pubic symphysis.
Pubic Angle: This is the angle formed by the convergence of the inferior rami of the pubis and ischium at the pubic symphysis. The width of this angle is a key morphological trait used to distinguish between male (narrower) and female (wider) skeletons.
Pubic Tubercle: This small, rounded projection is located on the upper border of the body of the pubis. It serves as the primary attachment point for the inguinal ligament, making it a vital landmark in hernia examinations.
Obturator Crest: This ridge extends from the pubic tubercle to the acetabular notch. It serves as the origin for the pubofemoral ligament, which reinforces the hip joint capsule.
Pectineal Line: Also known as the pecten pubis, this is a sharp ridge on the superior ramus of the pubis. It forms part of the pelvic brim and serves as an attachment for the pectineal ligament and the pectineus muscle covering.
Pectineal Surface: This is a triangular, flat surface on the superior ramus of the pubis, located between the pectineal line and the obturator crest. It provides the origin surface for the pectineus muscle.
Linia Arcuata / Arcuate Line: This smooth, rounded border is located on the internal surface of the ilium. It forms part of the linea terminalis, helping to define the pelvic inlet and separating the body of the ilium from the wing.
Spina Iliaca Ant.-Inf. (Anterior Inferior Iliac Spine): Located superior to the acetabulum and inferior to the anterior superior iliac spine, this projection is less prominent. It provides the origin point for the straight head of the rectus femoris muscle.
Iliac Fossa: This large, smooth, concave surface is located on the internal aspect of the ilium wing. It gives origin to the iliacus muscle, which is a primary flexor of the thigh.
Ant.-Sup. Iliac Spine (Anterior Superior Iliac Spine): This prominent projection marks the anterior extremity of the iliac crest. It is a palpable landmark used frequently in clinical measurements of leg length and serves as the attachment for the sartorius muscle and inguinal ligament.
Osteology and Function of the Pelvic Girdle
The hip bone, or os coxae, is a large, irregularly shaped bone that forms the pelvic girdle along with the sacrum and coccyx. Though it appears as a single unit in adulthood, it is developmentally formed by the fusion of three distinct bones: the ilium, ischium, and pubis. These three components meet and fuse within the acetabulum, the deep socket on the lateral aspect (not visible in this medial view) that articulates with the head of the femur. The medial view provided in the image is clinically significant because it reveals the internal surface of the pelvis, known as the true and false pelvis, which houses and protects the pelvic viscera.
The structural integrity of the hip bone is essential for its two primary functions: weight transmission and organ protection. The robust posterior section, specifically the auricular surface and iliac tuberosity, forms the Sacroiliac Joint with the vertebral column. This joint transfers the immense weight of the upper body and trunk down through the bony pelvis to the femurs during standing or to the ischial tuberosities during sitting. This architecture requires thick, dense bone and strong ligamentous attachments, which explains the roughness of landmarks like the iliac tuberosity.
Key physiological roles of the hip bone include:
- Mechanical Support: Transferring weight from the axial skeleton to the lower appendicular skeleton.
- Visceral Protection: Shielding the reproductive organs, urinary bladder, and parts of the digestive tract.
- Hematopoiesis: The marrow within the iliac crest is a primary site for red blood cell production and a common site for bone marrow biopsies.
- Muscle Attachment: Serving as an anchor for muscles that move the trunk and lower limbs.
The Three Components of the Hip Bone
The ilium is the largest and most superior portion of the hip bone, characterized by its fan-like wing or ala. The medial surface of the wing is dominated by the iliac fossa, a large concave area that houses the iliacus muscle. The superior border, the iliac crest, is bounded by the anterior and posterior superior iliac spines. These spines are critical palpable landmarks for clinicians; for example, the anterior superior iliac spine (ASIS) is used to locate the inguinal ligament and for standardizing leg length measurements.
The ischium forms the posteroinferior part of the hip bone. It is the strongest portion of the bone, designed to withstand significant compressive forces. The ischial spine and the ischial tuberosity are its most prominent features. The relationship between the ischial spine and the sciatic notches is vital in obstetrics, as the distance between the ischial spines helps determine the diameter of the mid-pelvis, which a fetus must pass through during birth. The ischial tuberosity is covered by the gluteus maximus when standing but becomes subcutaneous when sitting, bearing the body’s weight.
The pubis forms the anterior portion of the hip bone. It consists of a body and two rami (superior and inferior). The superior ramus helps form the Obturator Foramen, a large opening that lightens the weight of the hip bone while providing surface area for muscle attachment. The medial surface of the pubis joins the opposite pubis at the pubic symphysis. The morphology of the pubis, particularly the pubic angle and the length of the pubic ramus, is the most reliable indicator for sex determination in skeletal remains, with females typically exhibiting a wider angle and a more rectangular pubic body to facilitate childbirth.
In conclusion, understanding the detailed anatomy of the medial hip bone is fundamental for medical professionals. From the weight-bearing mechanics of the sacroiliac joint to the obstetrical importance of the pelvic inlet defined by the arcuate line, each labeled structure plays a specific role in human physiology. This view allows for a comprehensive study of the internal architecture that supports locomotion and protects vital pelvic organs.


{kind=link}