Understanding the skeletal architecture of the lower limb is fundamental for diagnosing traumatic injuries, degenerative diseases, and biomechanical dysfunctions. The bones of the leg provide the necessary structural rigidity to support the weight of the entire body while facilitating a complex range of motion required for ambulation, running, and jumping. This anterior view illustrates the primary osseous structures that constitute the lower extremity, highlighting the spatial relationships that define the functional anatomy of the thigh, knee, and lower leg.
Label-by-Label Explanation
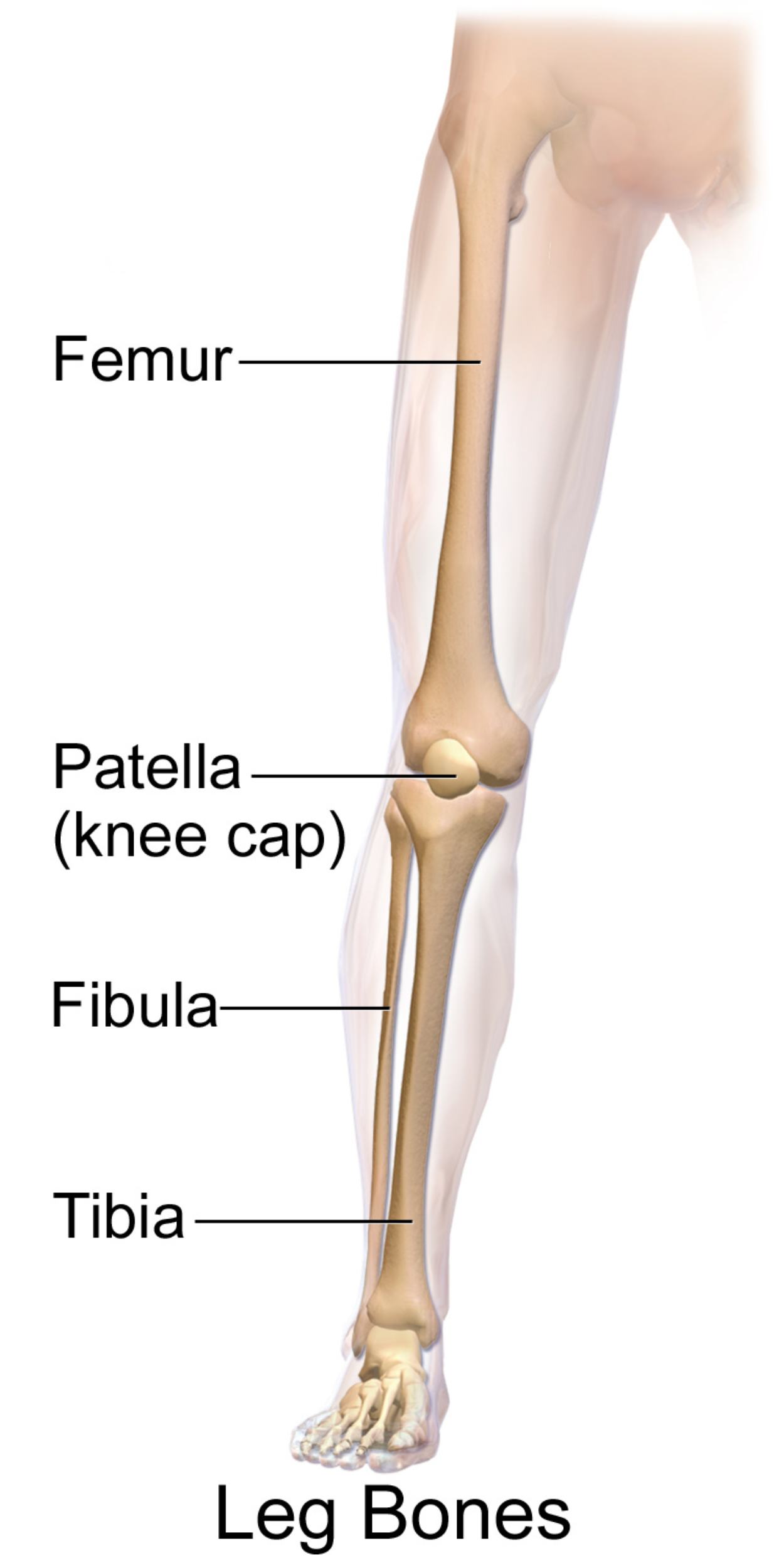
Femur
The femur is the longest and strongest bone in the human body, forming the skeletal framework of the thigh. It articulates proximally with the acetabulum of the pelvis and distally with the tibia and patella, acting as the primary transmitter of body weight from the torso to the lower leg. Clinically, the femoral neck and shaft are frequent sites of fractures, especially in geriatric populations or high-impact trauma cases.
Patella (knee cap)
The patella is the largest sesamoid bone in the body, embedded within the quadriceps tendon and situated at the anterior aspect of the knee joint. It functions as a biomechanical fulcrum, increasing the leverage and mechanical advantage of the quadriceps femoris muscle during knee extension. It also serves a protective role for the underlying tibiofemoral joint structures.
Fibula
The fibula is a slender bone located on the lateral side of the tibia and does not participate directly in weight-bearing at the knee joint. It serves primarily as an essential site for muscle and ligamentous attachment and forms the lateral malleolus at the ankle, providing lateral stability to the talocrural joint. Its proximal end, the head of the fibula, is a landmark for the common peroneal nerve.
Tibia
Commonly referred to as the shinbone, the tibia is the larger, medial bone of the lower leg and the second-longest bone in the body. It bears the vast majority of the body’s weight between the knee and the ankle joints. Its anterior border is subcutaneous and easily palpable, making it a common site for open fractures and stress injuries in athletes.
Anatomical Overview
The lower limb bones are organized into functional segments: the thigh (femoral region), the knee (patellar region), and the leg proper (crural region). In the anterior view, the alignment of these bones defines the mechanical axis of the lower extremity. The angle formed between the long axis of the femur and the tibia, known as the Q-angle, is a critical metric in orthopedic assessment, as deviations can lead to patellofemoral instability or accelerated joint wear.
The distal femur expands into medial and lateral condyles, which articulate with the flattened tibial plateau. Between these condyles lies the intercondylar notch, which houses the cruciate ligaments. The tibia and fibula are connected along their lengths by a thick interosseous membrane, which provides additional surface area for muscle attachment and helps distribute forces between the two bones.
Functional Significance
The bones visible in this anterior view are designed for both stability and mobility. The structural design of the femur allows it to withstand significant compressive and tensile forces during locomotion. The patella facilitates efficient knee extension by moving the pull of the quadriceps tendon away from the joint’s center of rotation, thereby increasing the torque produced by the muscle group.
In the lower leg, the tibia acts as the primary pillar of support. While the fibula is non-weight-bearing at its proximal end, it plays a vital role in the ankle mortise. The distal ends of the tibia and fibula form a stable hinge for the talus bone of the foot. This configuration ensures that the leg can handle the dynamic loads of gait while maintaining the necessary flexibility for navigating uneven terrain.
Clinical Relevance
Knowledge of these structures is essential for several clinical scenarios:
- Fracture Management: Recognizing the typical fracture patterns of the tibial shaft or the femoral neck is vital for emergency and orthopedic medicine.
- Joint Pathology: Osteoarthritis commonly affects the medial compartment of the knee (tibiofemoral joint), often visible as joint space narrowing on radiographs.
- Sports Medicine: Conditions such as Osgood-Schlatter disease involve the tibial tuberosity, where the patellar ligament attaches, frequently affecting adolescent athletes.
- Nerve Injury: The proximity of the common fibular nerve to the head of the fibula makes it vulnerable to compression or trauma, leading to foot drop.
Diagnostic and Educational Importance
For healthcare learners, the anterior view of the leg bones serves as a foundational map for physical examination. Palpable landmarks, such as the patella, the medial malleolus of the tibia, and the lateral malleolus of the fibula, are used to orient clinicians during musculoskeletal assessments. In radiology, these structures are the primary focus of lower extremity X-rays, CT scans, and MRIs.
Understanding the normal appearance and alignment of these bones allows for the identification of subtle abnormalities, such as stress fractures in the tibia or subluxation of the patella. For students, mastering the terminology and spatial orientation of the lower limb is a prerequisite for understanding the complex muscular and neurovascular systems that support and move these osseous structures.
In summary, the leg bones comprise a sophisticated weight-bearing system. The femur, patella, tibia, and fibula work in concert to provide leverage, protection, and stability. Clinical mastery of this anatomy is indispensable for any practitioner involved in musculoskeletal care, surgery, or rehabilitation.
Medical Learning Tips
- The fibula is always located on the lateral side of the lower leg and does not articulate with the femur.
- The patella is a sesamoid bone that acts as a fulcrum to increase quadriceps muscle efficiency.
- The tibia is the primary weight-bearing bone between the knee and the ankle joints.
- The distal ends of the tibia and fibula form the medial and lateral malleoli of the ankle.


{kind=link}