The proximal convoluted tubule (PCT) is a highly active segment of the nephron, responsible for reclaiming the vast majority of valuable substances from the initial filtrate. This article provides a detailed diagrammatic explanation of the substances reabsorbed and secreted by the PCT, highlighting the intricate cellular mechanisms that ensure essential nutrients and ions are returned to the bloodstream. Understanding the PCT’s multifaceted transport functions is fundamental to comprehending overall kidney physiology and the implications of its dysfunction in renal diseases.
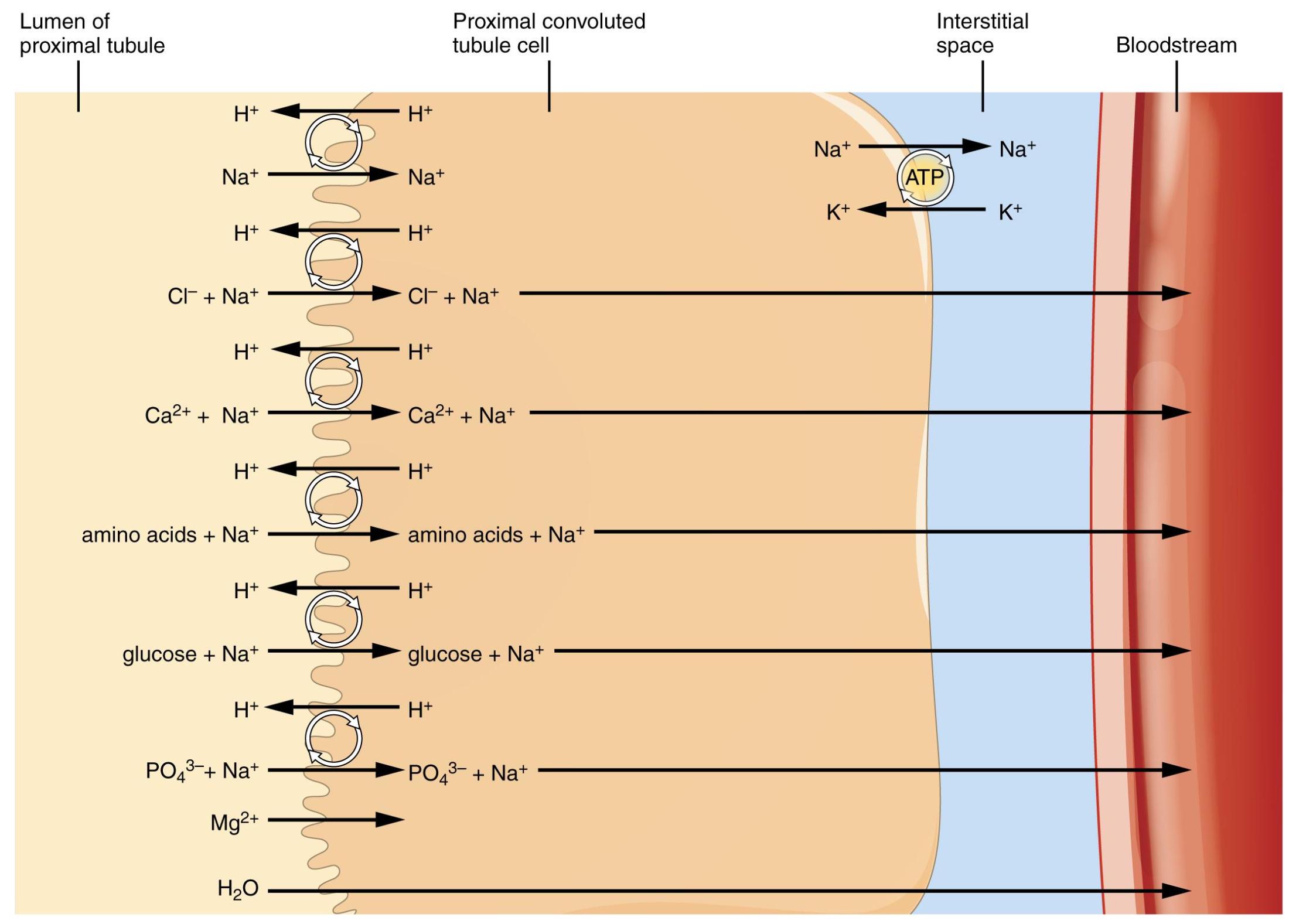
Lumen of proximal tubule: This is the inner space of the proximal convoluted tubule, containing the filtrate that has just been produced by the glomerulus. It is from this fluid that reabsorption occurs, returning substances to the blood.
Proximal convoluted tubule cell: These are the epithelial cells lining the PCT, characterized by extensive brush borders on their apical surface and numerous mitochondria. These features equip them for active transport and high metabolic activity, enabling efficient reabsorption and secretion.
Interstitial space: This is the fluid-filled space surrounding the renal tubule cells and the peritubular capillaries. Substances reabsorbed from the tubule move into this space before entering the bloodstream.
Bloodstream: This represents the peritubular capillaries, which are a network of blood vessels closely associated with the renal tubules. Reabsorbed substances from the interstitial space enter the bloodstream here to be returned to general circulation.
The proximal convoluted tubule (PCT) is truly a powerhouse within the nephron, performing an enormous amount of work to modify the glomerular filtrate. Unlike the relatively indiscriminate filtration at the glomerulus, the PCT selectively reclaims about 60-70% of the filtered water and solutes. This essential segment ensures that crucial nutrients, electrolytes, and bicarbonate are not lost in the urine, while also initiating the removal of certain waste products. The intricate cellular architecture of the PCT, with its specialized transporters and high energy demands, underpins its role as the kidney’s primary reabsorber. This diagram provides a clear visual representation of the diverse array of substances moving across the PCT cell.
The remarkable efficiency of the PCT stems from its highly specialized epithelial cells. These cells possess an extensive brush border on their luminal surface, vastly increasing the surface area for reabsorption. They are also packed with mitochondria, providing the abundant ATP required for active transport processes. The reabsorption of sodium ions (Na+) is a primary active transport event, driven by the Na+/K+-ATPase pump located on the basolateral membrane (facing the interstitial space). This pump maintains a low intracellular Na+ concentration, creating a gradient that facilitates the passive entry of Na+ from the tubular lumen into the cell. This sodium gradient is then leveraged to co-transport a multitude of other vital substances back into the cell and subsequently into the bloodstream.
Specifically, the diagram illustrates the co-transport of:
- Glucose + Na+: Nearly 100% of filtered glucose is reabsorbed here via sodium-glucose co-transporters (SGLTs).
- Amino acids + Na+: Similarly, the majority of filtered amino acids are reabsorbed through sodium-dependent co-transporters.
- PO43- + Na+: Phosphate is also reabsorbed, regulated by hormones like parathyroid hormone.
- Ca2+ + Na+ and Mg2+ + Na+: These ions are reabsorbed, contributing to electrolyte balance.
Furthermore, the PCT plays a critical role in acid-base balance by secreting hydrogen ions (H+) into the lumen, often in exchange for sodium, and reabsorbing bicarbonate (HCO3-). Chloride (Cl-) typically follows sodium passively. Water (H2O) reabsorption is also substantial, primarily driven by osmosis as solutes are moved from the tubule lumen into the peritubular capillaries. While the PCT is known for reabsorption, it also actively secretes certain organic acids and bases, drugs, and some waste products into the filtrate, contributing to their efficient excretion.
Dysfunction of the proximal convoluted tubule can lead to a variety of renal tubular disorders, significantly impacting overall health. For instance, Fanconi syndrome is a generalized disorder of PCT function, leading to impaired reabsorption of glucose, amino acids, phosphate, and bicarbonate, resulting in their excessive loss in the urine. Similarly, in uncontrolled diabetes mellitus, the glucose transporters in the PCT can become saturated, leading to glycosuria (glucose in the urine) as the reabsorptive capacity is exceeded. Understanding the specific transport mechanisms and the substances handled by the PCT is therefore indispensable for diagnosing and managing these complex conditions, ensuring the body maintains its vital homeostatic balance.


{kind=link}