The Ankle-Brachial Index (ABI) is a non-invasive diagnostic test used to assess vascular health by comparing blood pressure in the arms and legs. This procedure is the gold standard for detecting peripheral artery disease (PAD), a condition causing reduced blood flow to the limbs due to narrowed arteries. By utilizing a Doppler ultrasound device and standard pressure cuffs, clinicians can calculate a ratio that indicates the severity of arterial blockage, allowing for early intervention and management of cardiovascular risks.
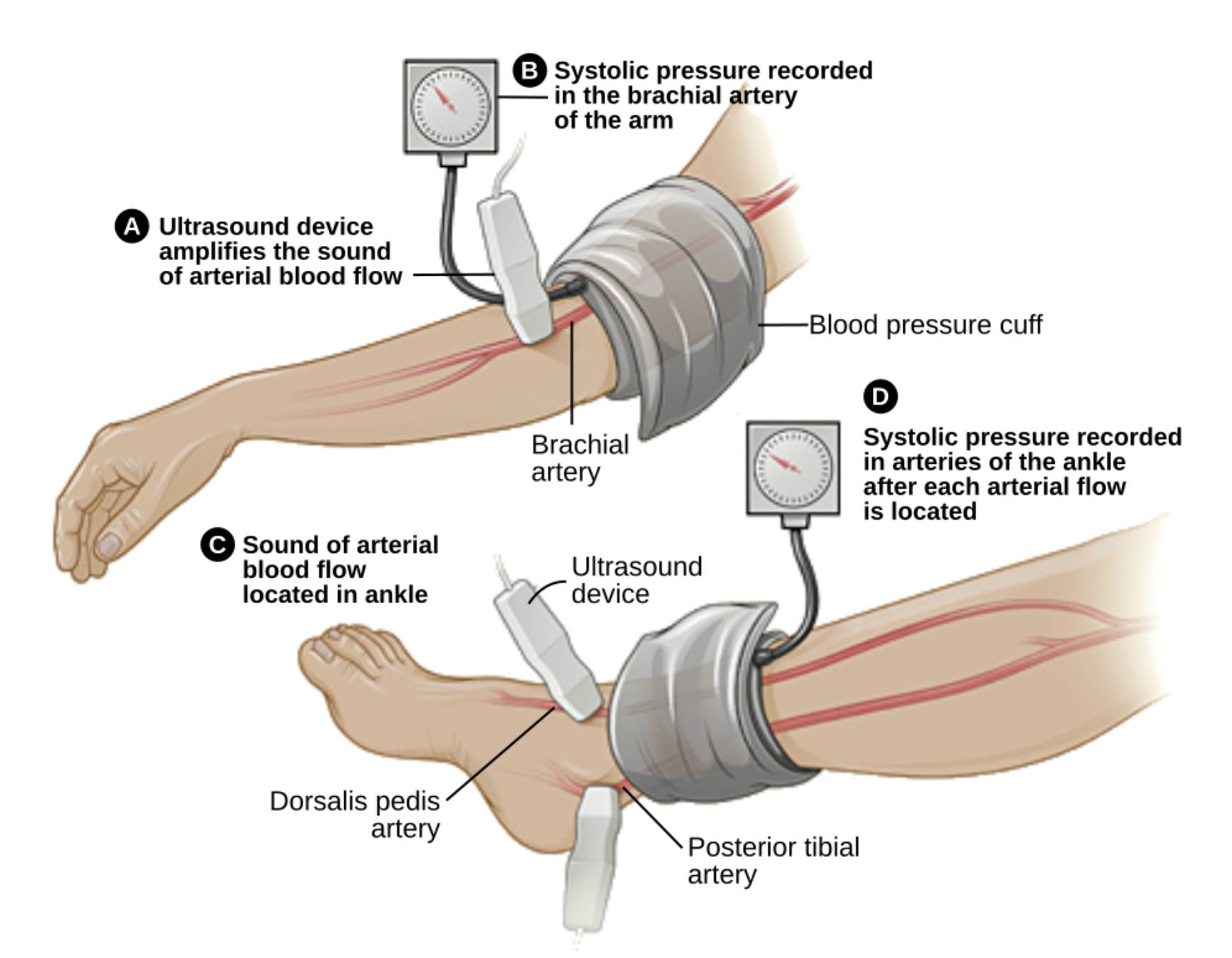
A Ultrasound device amplifies the sound of arterial blood flow: This handheld tool utilizes Doppler technology to detect the movement of red blood cells within the blood vessels. It converts the rhythmic flow of blood into an audible “whooshing” sound, allowing the clinician to identify the pulse even when it is too faint to be felt manually.
B Systolic pressure recorded in the brachial artery of the arm: This measurement captures the maximum arterial pressure during the heartbeat in the upper arm. It serves as the reference denominator for the ABI calculation, as upper extremity pressure typically reflects central aortic pressure in the absence of subclavian disease.
Blood pressure cuff: This pneumatic device is wrapped snugly around the limb and inflated to temporarily occlude blood flow. By slowly releasing the air while listening with the Doppler device, the clinician identifies the precise pressure at which blood flow resumes.
Brachial artery: Located in the upper arm, this major vessel is the standard site for systemic blood pressure monitoring. In the context of the ABI test, the higher of the two brachial systolic pressures (left vs. right) is used to calculate the final index.
C Sound of arterial blood flow located in ankle: This label indicates the process of using the Doppler probe to locate specific pulse points on the foot. Finding a strong auditory signal is essential for accurate pressure readings, particularly in patients with poor circulation where a pulse cannot be palpated.
Dorsalis pedis artery: Running across the top of the foot, this artery is a continuation of the anterior tibial artery. It is one of the two primary vessels in the foot used to measure distal blood pressure, helping to identify blockages in the lower leg.
D Systolic pressure recorded in arteries of the ankle after each arterial flow is located: This value represents the return of blood flow to the lower extremity after cuff deflation. The higher systolic pressure found between the two ankle arteries is used as the numerator in the ABI ratio to determine vascular patency.
Posterior tibial artery: Situated behind the inner ankle bone (medial malleolus), this artery supplies blood to the sole of the foot. Measuring pressure at this site ensures a comprehensive assessment, as arterial disease may affect the anterior and posterior vessels unevenly.
The Physiology of the Ankle-Brachial Index
The Ankle-Brachial Index is a simple yet powerful physiological assessment. In a healthy circulatory system, gravity and vessel resistance typically cause the blood pressure in the ankles to be slightly higher than or equal to the pressure in the arms while the patient is lying down. Therefore, a normal ABI ratio is usually between 1.0 and 1.4. When cholesterol plaque builds up in the arteries of the legs, it creates resistance that lowers the pressure downstream. Consequently, if the blood pressure in the ankle is significantly lower than in the arm, it indicates a blockage somewhere between the heart and the foot.
The procedure is generally performed with the patient in a supine position to negate the effects of hydrostatic pressure. After the clinician gathers the systolic pressures from both arms and both ankles (using the dorsalis pedis and posterior tibial arteries), the ratio is calculated. This is done by dividing the higher systolic pressure of the ankle by the higher systolic pressure of the arm. This mathematical approach provides a quantitative measurement of blood flow that correlates strongly with the degree of arterial narrowing.
Common risk factors that necessitate an ABI test include:
- History of smoking or tobacco use.
- Diabetes mellitus.
- Hypertension (high blood pressure).
- High cholesterol (hyperlipidemia).
- Age over 50 with a history of diabetes or smoking, or age over 70 regardless of history.
Peripheral Artery Disease: Pathopathology and Symptoms
The primary condition diagnosed by the ABI test is Peripheral Artery Disease (PAD). PAD is a manifestation of systemic atherosclerosis, a process where fatty deposits, calcium, and fibrous tissue accumulate within the arterial walls. Over time, these plaques harden and narrow the lumen of the vessel (stenosis), restricting the flow of oxygen-rich blood to the muscles and tissues of the legs. While PAD can remain asymptomatic in its early stages, it is a progressive disease that signals a high risk for heart attack and stroke.
As the disease advances, patients often experience a symptom known as intermittent claudication. This is characterized by cramping, pain, or tiredness in the leg muscles (calves, thighs, or buttocks) that occurs during physical activity and resolves with rest. The pain is caused by ischemia; the muscles require more oxygen during walking than the narrowed arteries can supply. In severe cases, the blood supply may become so compromised that the tissue dies, leading to non-healing ulcers or gangrene, a condition known as Critical Limb Ischemia (CLI).
Interpreting Diagnostic Results
The interpretation of the Ankle-Brachial Index is categorized into specific ranges. A result of 0.90 to 0.99 is considered borderline, while a ratio of less than 0.90 is diagnostic for PAD. The lower the number, the more severe the obstruction; for example, a ratio below 0.50 usually indicates severe ischemia and a potential threat to limb viability. Conversely, a ratio greater than 1.40 can indicate non-compressible arteries, often seen in elderly patients or those with long-standing diabetes, where the vessel walls have become calcified and stiff.
Conclusion
The Ankle-Brachial Index is an indispensable screening tool in modern cardiovascular medicine. By relying on the fundamental principles of hemodynamics and Doppler ultrasound, it provides a safe, rapid, and accurate assessment of lower extremity blood flow. Early detection of abnormal ABI values allows healthcare providers to initiate lifestyle changes and medical therapies that not only preserve limb function but also significantly reduce the patient’s overall cardiovascular risk.


{kind=link}