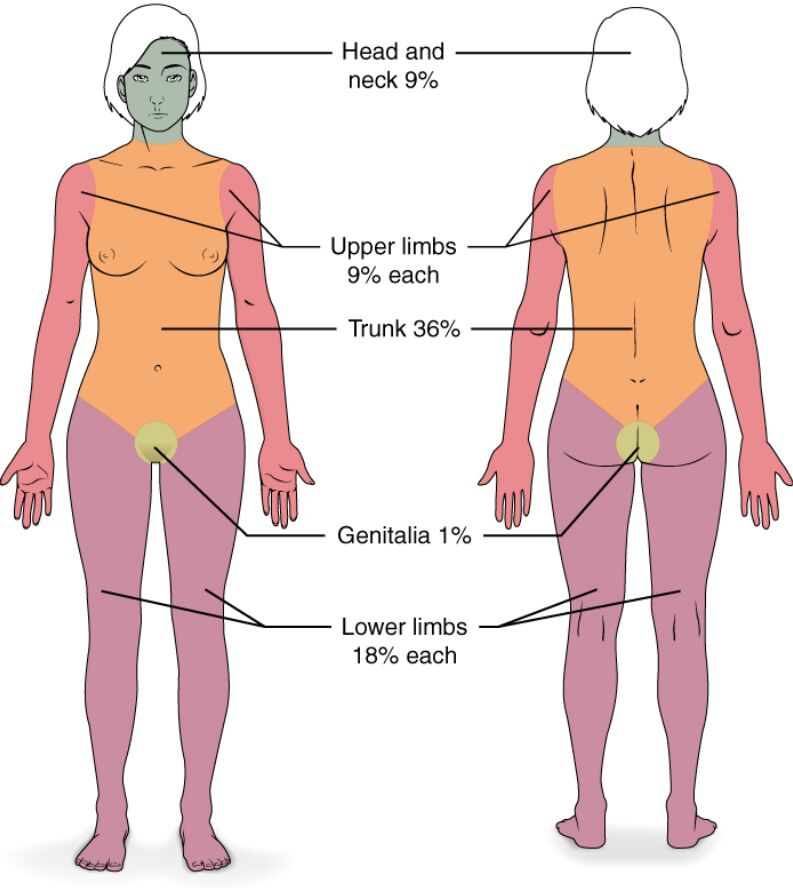
This diagram illustrates the Rule of Nines, a crucial tool for rapidly estimating the total body surface area (TBSA) affected by burns in adults. This standardized method assigns specific percentage values to different anatomical regions, providing an immediate assessment that guides critical decisions regarding fluid resuscitation, pain management, and the need for specialized burn care. Understanding this calculation is fundamental for emergency medical professionals.
Labels Explanation:
Head and neck 9%: This region encompasses the entire head and neck area, accounting for 9% of the total body surface area. Burns to this area, regardless of size, are often considered critical due to proximity to the airway and potential for inhalation injury.
Upper limbs 9% each: Each arm, including the hand, represents 9% of the total body surface area. This means both upper limbs together account for 18%, and burns to these areas can significantly impact mobility and function.
Trunk 36%: The trunk, including the chest, abdomen, and back, constitutes the largest single region, accounting for 36% of the total body surface area (18% for the anterior trunk and 18% for the posterior trunk). Extensive burns here necessitate aggressive fluid management.
Genitalia 1%: The genital area represents a small but critical 1% of the total body surface area. Burns to this region, even if small, are considered highly sensitive and often require specialized care due to pain and risk of infection.
Lower limbs 18% each: Each leg, including the foot, accounts for 18% of the total body surface area. Both lower limbs together comprise 36%, and deep burns in these areas can lead to significant fluid loss and long-term functional impairment.
Introduction to Estimating Burn Size
Accurately estimating the size of a burn is one of the most critical initial steps in the management of burn injuries. The total body surface area (TBSA) affected by a burn directly dictates the severity of the injury, guiding crucial decisions related to fluid resuscitation, pain control, and the need for transfer to a specialized burn center. Incorrect estimation can lead to either under-resuscitation, risking hypovolemic shock, or over-resuscitation, which can cause complications like fluid overload and acute respiratory distress syndrome. Therefore, methods like the Rule of Nines, as depicted, provide a standardized and rapid approach to this vital assessment.
The Rule of Nines is a widely adopted technique, particularly in pre-hospital and emergency department settings, due to its simplicity and ease of application. It divides the adult body into anatomical regions, each representing a multiple of 9% of the total body surface area. While it provides a quick estimate, it’s important to note that this rule is designed for adults and may not be accurate for children, whose body proportions differ significantly. For pediatric patients, the Lund-Browder chart is often preferred as it accounts for age-related variations in body proportions.
Key reasons for accurate burn size estimation include:
- Fluid Resuscitation: Determining the amount of intravenous fluids needed to prevent shock.
- Burn Center Referral: Guiding decisions on whether specialized burn care is required.
- Prognosis: Influencing the overall outlook and potential for complications.
- Pain Management: Informing appropriate analgesic strategies.
- Documentation: Providing a standardized record for medical and legal purposes.
Beyond the Rule of Nines, other methods such as the “palm method” (where the patient’s palm, excluding fingers, represents approximately 1% TBSA) can be used for smaller, scattered burns. Regardless of the method, precision in burn size estimation is paramount for delivering optimal care and improving patient outcomes.
The Clinical Significance of Burn Size
The size of a burn injury, specifically the Total Body Surface Area (TBSA) affected, is a primary determinant of a burn’s severity and subsequent patient management. Extensive burns trigger a systemic inflammatory response, leading to significant fluid shifts and electrolyte imbalances. When more than approximately 15-20% TBSA is involved in second-degree (partial thickness) or third-degree (full thickness) burns, patients are at high risk of developing burn shock. This is a form of hypovolemic shock caused by massive fluid loss from the damaged capillaries into the interstitial spaces, leading to decreased cardiac output and organ hypoperfusion.
Accurate TBSA calculation is essential for guiding fluid resuscitation, which is a cornerstone of initial burn management. Formulas like the Parkland formula are commonly used to calculate the volume of intravenous fluids (typically Lactated Ringer’s solution) required over the first 24 hours post-burn, with half of the total volume given in the first 8 hours and the remaining half over the next 16 hours. Inadequate fluid resuscitation can lead to irreversible shock and multi-organ failure, while over-resuscitation can cause pulmonary edema, abdominal compartment syndrome, and other complications. Furthermore, TBSA is a major criterion for determining the need for transfer to a specialized burn center, where comprehensive multidisciplinary care, including advanced wound care, nutritional support, and rehabilitative services, can be provided.
Applying the Rule of Nines in Practice
The Rule of Nines, while a rapid estimation tool, should be applied systematically to ensure accuracy. For an adult, the body is divided as follows: the entire head and neck account for 9%; each upper limb (arm) is 9%; the entire trunk is 36% (18% for the anterior surface and 18% for the posterior surface); each lower limb (leg) is 18%; and the genital area accounts for the remaining 1%. When assessing a burn, only second-degree (partial-thickness) and third-degree (full-thickness) burns are included in the TBSA calculation, as first-degree burns (like a superficial sunburn) do not cause significant fluid shifts.
Consider a scenario where an adult patient has full-thickness burns covering their entire left arm, the front of their trunk, and their head and neck. Using the Rule of Nines: the left arm contributes 9%, the front of the trunk contributes 18%, and the head and neck contribute 9%. The total TBSA burned would be 9% + 18% + 9% = 36%. This calculation would immediately inform the medical team about the severity of the injury and the aggressive fluid resuscitation and advanced care required. While practical, it’s crucial for healthcare providers to understand that the Rule of Nines is an estimation and continuous reassessment of the patient’s condition and fluid balance is necessary. For irregular or patchy burns, the palm method can supplement the Rule of Nines to refine the estimation, enhancing the precision of the initial assessment.
The Rule of Nines is an indispensable tool in emergency medicine and burn care, providing a rapid and standardized method for assessing the extent of burn injuries in adults. This quick estimation of Total Body Surface Area (TBSA) is fundamental for initiating appropriate fluid resuscitation, guiding decisions for specialized burn center referral, and ultimately influencing the overall prognosis of burn patients. Mastery of this technique is crucial for healthcare professionals involved in the immediate management of burn trauma, ensuring that vital, life-saving interventions are delivered effectively and efficiently.


{kind=link}