Malaria remains one of the most significant mosquito-borne infectious diseases worldwide, caused by protozoan parasites of the genus Plasmodium that undergo a complex life cycle involving both human and mosquito hosts. Diagnosis often relies on microscopic examination of Giemsa-stained blood smears, where different developmental stages of the parasite can be identified within erythrocytes. The provided image combines a histological section showing a sporozoite with a peripheral blood smear displaying ring forms, young trophozoites, and a schizont, offering a comprehensive educational view of key Plasmodium stages critical for accurate laboratory diagnosis and understanding the parasite’s intraerythrocytic development.
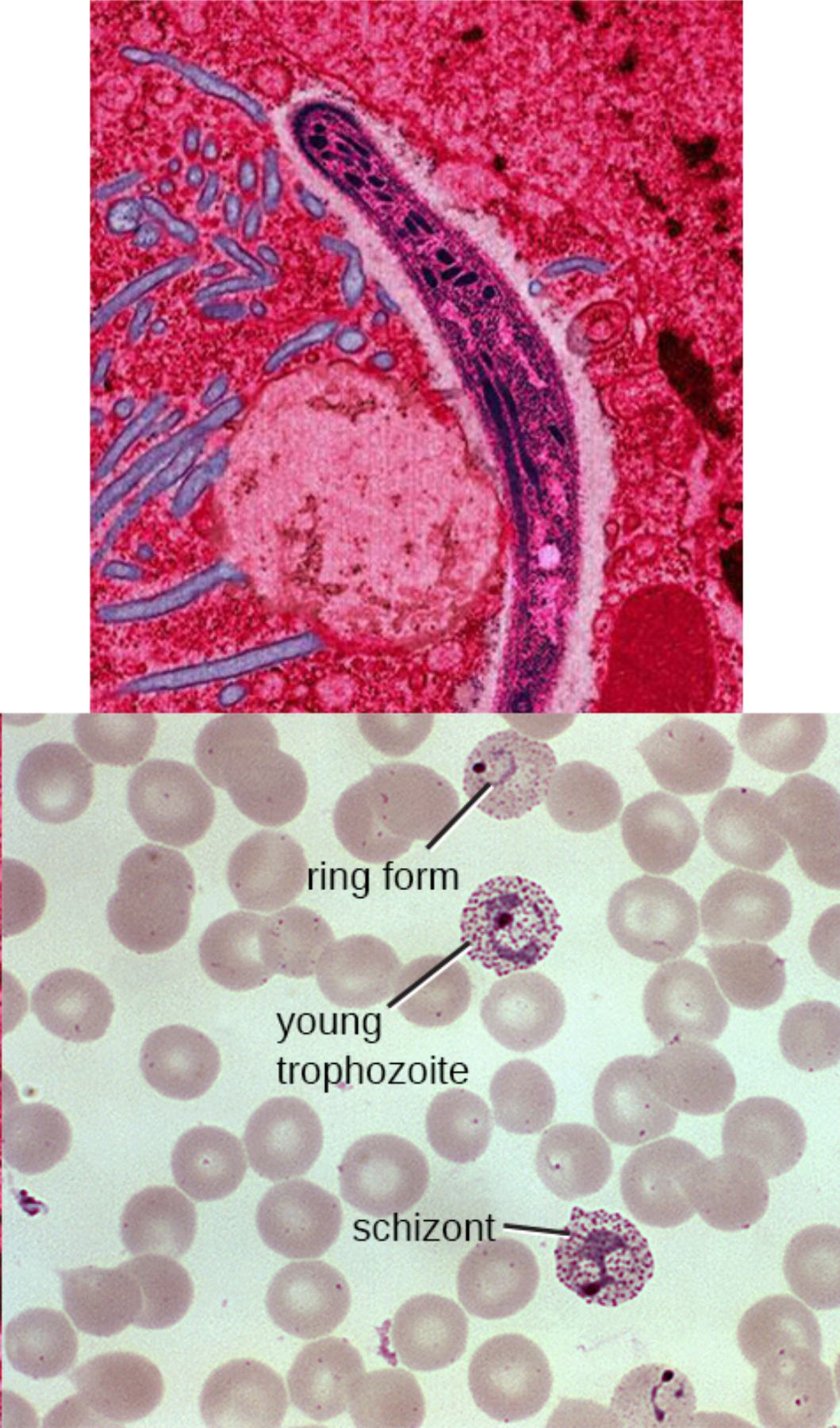
Sporozoite is the elongated, banana-shaped or curved structure visible in the upper panel within a tissue section, representing the infective form injected by an Anopheles mosquito during a blood meal. Sporozoites are motile and rapidly travel through the bloodstream to invade hepatocytes in the liver, initiating the pre-erythrocytic stage of infection. In the image, the sporozoite appears dark purple against the pink tissue background, highlighting its characteristic slender morphology with a pointed end.
Ring form is labeled in the lower blood smear panel as a small, ring-like structure inside a red blood cell with a central clear area and peripheral chromatin dot. This early trophozoite stage results from merozoite invasion of erythrocytes and represents the beginning of the blood-stage cycle. Ring forms are the most commonly observed stage in peripheral blood smears and are diagnostic for Plasmodium infection, appearing as delicate rings with minimal cytoplasm.
Young trophozoite appears as a slightly larger intraerythrocytic form with more visible cytoplasm and chromatin compared to the ring stage. At this stage, the parasite begins active metabolism and growth within the red blood cell, often showing amoeboid movement. The label points to a developing form that has progressed beyond the simple ring, indicating active intraerythrocytic maturation before schizogony.
Schizont is the mature, multi-nucleated stage labeled in the lower panel, characterized by multiple merozoites clustered within a single red blood cell. Schizonts represent the culmination of asexual replication inside erythrocytes, eventually rupturing to release new merozoites that infect additional red blood cells. In the image, the schizont shows numerous dark chromatin dots arranged in a cluster, typical of mature forms seen in certain Plasmodium species.
Life Cycle of Plasmodium and Stages in Blood Smears
The Plasmodium life cycle alternates between sexual reproduction in the mosquito and asexual reproduction in the human host. After sporozoites enter the human body, they undergo exoerythrocytic schizogony in the liver before releasing merozoites into the bloodstream. These merozoites invade erythrocytes, initiating the erythrocytic cycle visible in blood smears as ring forms, trophozoites, schizonts, and eventually gametocytes. The image effectively illustrates both the liver-stage sporozoite and key blood-stage forms.
Ring forms and young trophozoites are the predominant stages observed in peripheral blood during early infection, while schizonts are more commonly seen in severe cases or with certain species. Accurate identification of these stages helps determine the Plasmodium species and guides treatment decisions. The upper panel shows tissue invasion by sporozoites, while the lower panel demonstrates the intraerythrocytic development that causes clinical symptoms through periodic red blood cell rupture and release of merozoites.
- Ring forms typically measure 1/5 to 1/3 the diameter of the red blood cell.
- Young trophozoites show increasing cytoplasmic volume and irregular shape.
- Schizonts contain 8–24 merozoites depending on the Plasmodium species.
Diagnostic Features of Malaria in Blood Smears
Microscopic examination of thick and thin blood smears remains the gold standard for malaria diagnosis. Thick smears concentrate parasites for detection of low parasitemia, while thin smears allow species identification based on morphology. The labeled stages in the image—ring form, young trophozoite, and schizont—provide classic examples used by laboratory technicians worldwide to diagnose and differentiate Plasmodium species such as P. falciparum, P. vivax, P. ovale, and P. malariae.
P. falciparum is characterized by multiple ring forms per cell, appliqué forms, and the absence of schizonts in peripheral blood. In contrast, P. vivax and P. ovale often show enlarged erythrocytes and Schüffner’s dots. The schizont shown in the image is typical of non-falciparum species where all stages are visible in peripheral blood. Proper staining with Giemsa highlights chromatin (red-purple) and cytoplasm (blue), making parasite structures stand out against the pink-red blood cells.
- Thick smears are more sensitive for screening, while thin smears are essential for species identification.
- Parasitemia percentage is calculated by counting infected red blood cells in thin smears.
- Repeat smears may be necessary if initial results are negative but clinical suspicion remains high.
Clinical Importance and Management of Malaria
Malaria presents with cyclic fever, chills, headache, and fatigue corresponding to the synchronous rupture of infected erythrocytes. Severe malaria, most commonly caused by P. falciparum, can lead to cerebral malaria, severe anemia, respiratory distress, and multi-organ failure. Early diagnosis through blood smear examination, as illustrated in the image, is critical for timely initiation of antimalarial therapy and prevention of complications.
Treatment depends on the species, severity, and drug resistance patterns in the region. Artemisinin-based combination therapies are first-line for uncomplicated P. falciparum, while chloroquine remains effective against sensitive non-falciparum species. Primaquine is used for radical cure of P. vivax and P. ovale to eliminate liver hypnozoites. Supportive care and monitoring for complications are essential in severe cases.
Prevention strategies include insecticide-treated bed nets, indoor residual spraying, and antimalarial chemoprophylaxis for travelers. Vaccine development has progressed with RTS,S and R21 vaccines targeting the sporozoite stage, aiming to interrupt the pre-erythrocytic phase shown in the upper panel of the image.
- Travel history to endemic areas is a key clue in non-endemic regions.
- Pregnant women and young children are at highest risk for severe disease.
- Drug resistance monitoring is essential for effective treatment guidelines.
Laboratory Techniques and Species Differentiation
Accurate species identification from blood smears requires careful examination of parasite morphology, red blood cell size, and presence of stippling. The ring form, young trophozoite, and schizont labeled in the image represent progressive stages of intraerythrocytic development. P. falciparum typically shows delicate rings and banana-shaped gametocytes, while P. vivax displays larger trophozoites with amoeboid shapes and Schüffner’s dots.
Rapid diagnostic tests detecting histidine-rich protein 2 or lactate dehydrogenase provide quick results but should be confirmed with microscopy when possible. Molecular methods such as PCR offer high sensitivity and species specificity but are not routinely available in resource-limited settings. The image serves as an excellent teaching tool for training microscopists in recognizing these critical diagnostic stages.
Understanding the morphological features shown in the blood smear and tissue section is fundamental for medical laboratory professionals, clinicians, and students studying tropical medicine. Mastery of these stages enables rapid diagnosis, appropriate treatment, and effective public health responses to reduce the global burden of malaria.


{kind=link}