This professional cadaveric dissection provides a high-resolution lateral view of the right neck and shoulder region, illustrating the intricate relationships between major vascular channels, neural networks, and skeletal muscles. By examining these structures in situ, clinicians and students can better visualize the pathways of the common carotid artery and the branches of the brachial plexus as they transition from the thoracic outlet toward the upper extremity.
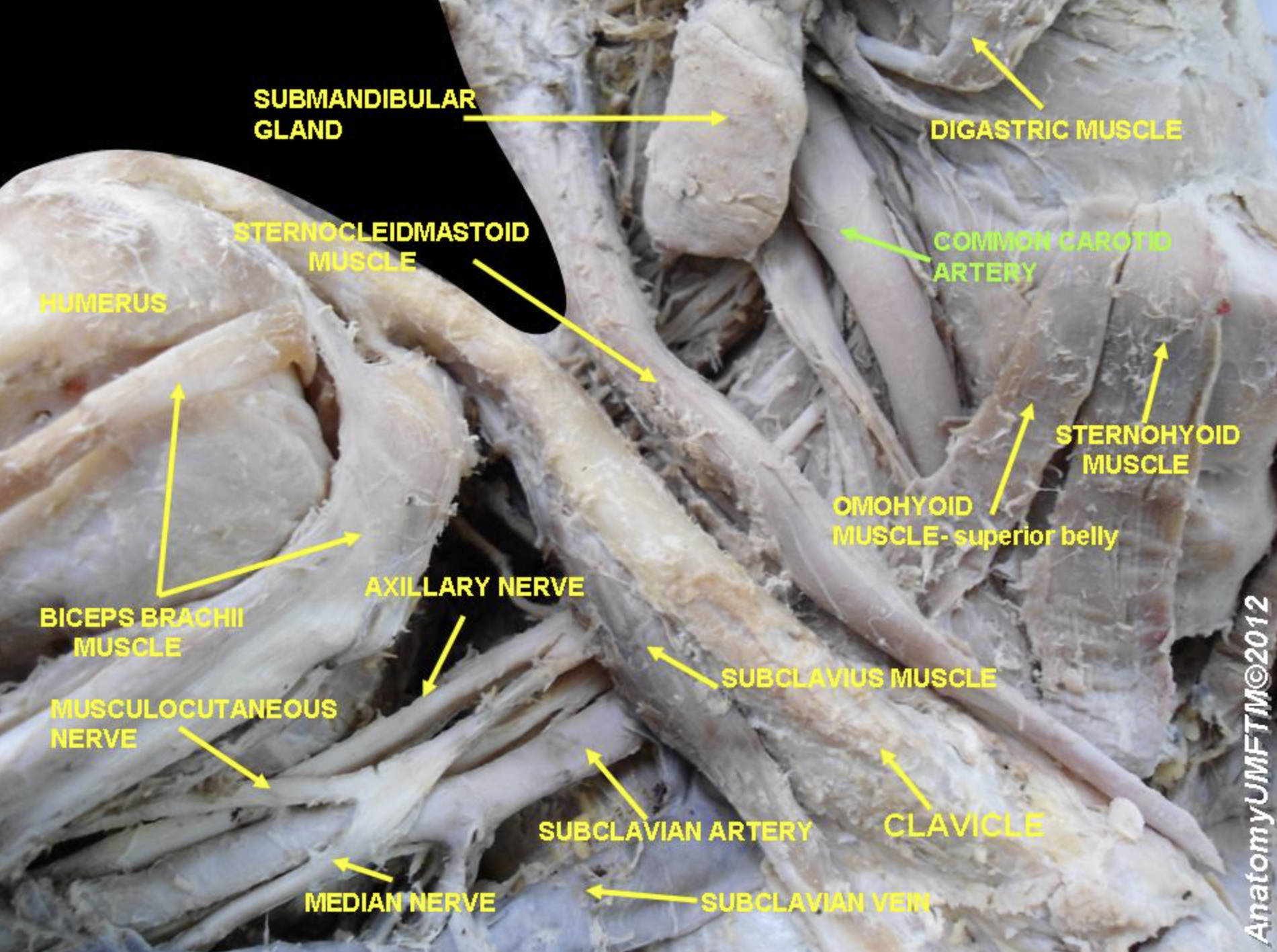
SUBMANDIBULAR GLAND: This is a major salivary gland located within the submandibular triangle of the neck, just below the mandible. It is responsible for producing approximately 70% of the body’s unstimulated saliva, which is essential for oral hygiene and the initial stages of chemical digestion.
DIGASTRIC MUSCLE: A small but important muscle consisting of an anterior and posterior belly connected by an intermediate tendon. It functions to depress the mandible and elevate the hyoid bone, playing a critical role in the complex movements required for swallowing and speech.
COMMON CAROTID ARTERY: This is the primary vessel responsible for delivering oxygenated blood to the head and neck. On the right side, it typically originates from the brachiocephalic trunk and ascends within the carotid sheath alongside the internal jugular vein and vagus nerve.
STERNOCLEIDOMASTOID MUSCLE: A prominent, superficial muscle of the neck that serves as a landmark for dividing the neck into anterior and posterior triangles. Its contraction allows for the rotation of the head to the opposite side and the flexion of the cervical spine.
STERNOHYOID MUSCLE: This long, thin muscle belongs to the infrahyoid “strap” muscle group and is situated anterior to the larynx and trachea. It acts to depress the hyoid bone after it has been elevated during the swallowing process.
OMOHYOID MUSCLE- superior belly: This specific segment of the omohyoid muscle attaches to the hyoid bone and descends toward the intermediate tendon. It works in conjunction with other infrahyoid muscles to stabilize the hyoid bone and the underlying cervical fascia.
HUMERUS: The humerus is the largest bone of the upper limb, forming the structural core of the arm. It provides attachment points for numerous muscles, including the deltoid and rotator cuff, and articulates with the scapula to form the glenohumeral joint.
BICEPS BRACHII MUSCLE: A prominent muscle located in the anterior compartment of the arm that features both a long and a short head. It is the primary supinator of the forearm and a powerful flexor of the elbow joint.
AXILLARY NERVE: Originating from the posterior cord of the brachial plexus, this nerve passes through the quadrangular space to reach the shoulder. It provides essential motor innervation to the deltoid and teres minor muscles, as well as sensory input to the skin over the lower deltoid region.
MUSCULOCUTANEOUS NERVE: This nerve arises from the lateral cord of the brachial plexus and typically pierces the coracobrachialis muscle. It provides motor control to the muscles of the anterior arm and continues into the forearm as a sensory nerve.
SUBCLAVIUS MUSCLE: A small, triangular muscle located in the narrow space between the first rib and the inferior surface of the clavicle. It helps to depress and stabilize the clavicle during various movements of the shoulder girdle.
SUBCLAVIAN ARTERY: This major systemic artery originates from the brachiocephalic trunk on the right and supplies the entire upper limb with oxygenated blood. As it passes over the first rib, it changes its name to the axillary artery before continuing down the arm.
CLAVICLE: Frequently referred to as the collarbone, this S-shaped bone acts as a strut that keeps the upper limb away from the thorax. It also serves as a protective barrier for the underlying neurovascular bundle as it enters the axillary region.
SUBCLAVIAN VEIN: This large vessel is the primary pathway for venous return from the upper limb back toward the heart. It lies anterior to the subclavian artery and joins the internal jugular vein to form the brachiocephalic vein behind the sternoclavicular joint.
MEDIAN NERVE: Formed by the convergence of the lateral and medial cords of the brachial plexus, this nerve travels down the medial aspect of the arm. It is critical for the motor function of most forearm flexors and provides sensory innervation to several fingers and the palm.
The anatomy of the right neck and shoulder region is a masterpiece of spatial organization, where vital life-sustaining structures are packed into a relatively small area. The transition from the cervical region to the upper limb involves the passage of nerves and vessels through a series of narrow “gateways,” such as the interscalene space and the axillary inlet. Understanding these boundaries is vital for managing clinical conditions ranging from thoracic outlet syndrome to complex upper-limb trauma.
In this dissection, we see how the muscular architecture provides both movement and protection. Muscles like the sternocleidomastoid not only move the head but also serve as protective layers for the deep neurovascular bundles. Similarly, the clavicle acts as a bony shield for the subclavian vessels and the nerves of the arm, which are vulnerable to compression or injury during high-impact trauma to the chest and shoulder.
The coordination of different physiological systems in this region is remarkable:
- The circulatory system ensures a constant supply of nutrients to the brain and upper limbs via the carotid and subclavian arteries.
- The nervous system provides the electrical signaling required for complex hand movements and sensory feedback.
- The musculoskeletal system offers the mechanical levers and protective cavities necessary for life and locomotion.
- The glandular system (submandibular gland) contributes to the initial stages of the digestive process.
A thorough understanding of these structures is the cornerstone of safe surgical and anesthetic practice. For example, during the administration of an interscalene block for shoulder surgery, an anesthesiologist must be able to visualize the exact position of the brachial plexus relative to the scalene muscles and the subclavian artery. Cadaveric images like the one provided here offer an invaluable three-dimensional perspective that textbooks alone cannot fully convey, highlighting the natural variations and depth of human anatomy.
The complexity shown in this lateral view of the right neck underscores the integrated nature of human physiology. From the salivary secretions of the submandibular gland to the motor impulses traveling through the median nerve, every structure plays a specific, vital role. By mastering these anatomical details, medical professionals are better equipped to diagnose pathologies, perform life-saving interventions, and improve patient outcomes through informed clinical decision-making.


{kind=link}