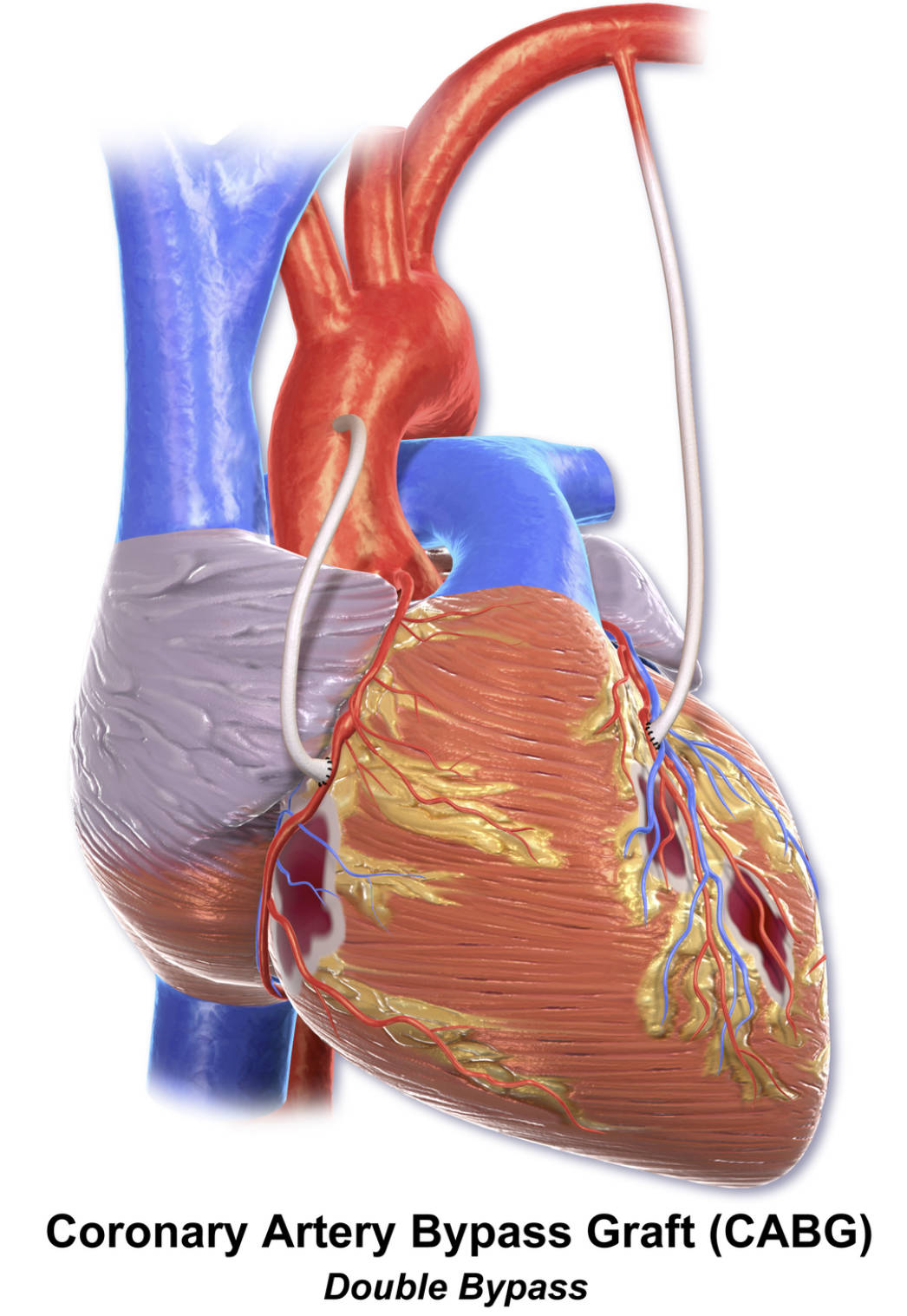
This diagram provides a clear visual representation of a double Coronary Artery Bypass Graft (CABG) procedure, illustrating how two distinct grafts are utilized to bypass significant blockages in two different coronary arteries. This surgical approach is crucial for patients experiencing multi-vessel coronary artery disease, where more than one major artery supplying the heart muscle is severely compromised. Understanding the principles and execution of a double bypass, as depicted, is essential for appreciating its role in restoring critical blood flow and improving cardiac function.
Introduction to Double Bypass CABG
Coronary Artery Bypass Graft (CABG) surgery is a highly effective treatment for severe coronary artery disease (CAD), a condition characterized by the accumulation of atherosclerotic plaque within the heart’s arteries. When these blockages become critical, they restrict blood flow to the myocardium, leading to symptoms like angina, shortness of breath, and an elevated risk of heart attack. A “double bypass” CABG, as precisely shown in this diagram, involves the creation of two new pathways to circumvent significant obstructions in two separate coronary arteries. This surgical intervention is a tailored solution for patients with multi-vessel CAD.
The primary goal of a double bypass is to restore robust blood flow to two distinct regions of the heart muscle that are suffering from insufficient oxygen supply due to severe blockages. This intricate procedure utilizes healthy blood vessels, typically harvested from the patient’s own body—such as the internal mammary artery from the chest and/or segments of the saphenous vein from the leg—as bypass grafts. These grafts are then surgically connected to the coronary arteries, effectively creating detours around the diseased segments. The result is improved oxygenation of the affected heart muscle, leading to significant symptom relief, enhanced cardiac function, and an improved quality of life.
The decision to perform a double bypass is made after a comprehensive diagnostic assessment, including coronary angiography, which accurately maps the location and severity of all arterial blockages. This personalized surgical strategy is critical for optimizing outcomes in patients with more widespread coronary artery disease than can be addressed by a single bypass.
Key indications that may lead to a double bypass CABG include:
- Significant blockages in two major coronary arteries: When two distinct arteries have critical stenoses.
- Persistent angina or other ischemic symptoms: Not adequately controlled by medication or less invasive procedures.
- Left Main Coronary Artery (LMCA) disease with additional vessel involvement: Though LMCA disease alone often leads to a single bypass to its branches, if another major vessel is also blocked, a double bypass becomes necessary.
- Complex or diffuse disease: When blockages are not suitable for percutaneous coronary intervention (PCI).
- Diabetes mellitus with multi-vessel CAD: CABG often shows superior long-term results in these patients.
These factors guide the cardiac surgical team in formulating the most appropriate treatment plan.
Understanding Multi-Vessel Coronary Artery Disease
The heart’s demand for oxygen and nutrients is met by the coronary arteries. The main arteries include the left anterior descending (LAD) artery, the circumflex artery (LCx), and the right coronary artery (RCA). Each of these vessels, along with their branches, supplies specific regions of the myocardium. In multi-vessel coronary artery disease, atherosclerotic plaque has accumulated to a significant extent in two or more of these major arteries. This widespread accumulation leads to multiple critical narrowings or blockages, severely compromising the heart’s ability to pump blood effectively and receive adequate oxygen.
When two distinct arteries are critically narrowed, the affected regions of the heart muscle experience ischemia. This reduced blood flow can lead to more widespread symptoms and a higher risk of adverse cardiac events, including heart attacks and heart failure. A double bypass is therefore specifically designed to address these two separate areas of concern, ensuring that both compromised regions receive a renewed and sufficient blood supply. By restoring flow to multiple vessels, the overall function of the heart can be significantly improved, and the burden of the disease lessened.
The Double Bypass Procedure: Graft Selection and Implementation
A double bypass CABG involves the meticulous creation of two new conduits to bypass two specific blockages in the coronary arteries. This open-heart procedure is typically performed under general anesthesia, and often involves connecting the patient to a heart-lung machine (cardiopulmonary bypass) to keep the blood circulating while the heart is temporarily stopped.
Commonly used graft vessels for a double bypass include:
- Internal Mammary Artery (IMA): The left internal mammary artery (LIMA) is frequently used as one of the grafts, often directed to bypass a blockage in the left anterior descending (LAD) artery. The LIMA is left attached at its origin from the subclavian artery and is then sewn onto the LAD beyond the obstruction. Its arterial nature provides excellent long-term patency.
- Saphenous Vein Graft (SVG): A segment of the saphenous vein, usually harvested from the leg, serves as the second graft. This vein segment is prepared, reversed (to ensure valve patency), and typically connected from the aorta to the second blocked coronary artery (e.g., the right coronary artery or a major branch of the circumflex artery) distal to its obstruction. The diagram clearly illustrates these two distinct grafts in place.
- Radial Artery: In some cases, the radial artery from the arm may be used as an alternative or additional graft.
The surgical team carefully selects the appropriate grafts and precisely performs the anastomoses (connections) to ensure robust and durable new blood flow pathways around the diseased segments.
Recovery and Long-Term Outlook After Double Bypass
Recovery from a double bypass CABG is a structured and often intensive process. Patients will spend time in an intensive care unit (ICU) immediately after surgery for close monitoring, followed by a transition to a standard hospital ward. Pain management, wound care for both the chest incision and graft harvest sites, and gradual physical mobilization are crucial components of the early recovery phase. Participation in a cardiac rehabilitation program is highly recommended and beneficial. These programs offer supervised exercise, dietary counseling, and comprehensive education on managing cardiovascular risk factors, all tailored to facilitate optimal recovery and improve long-term health.
The long-term outlook for patients who undergo a double bypass CABG is generally favorable, with significant improvements in symptoms, quality of life, and often, an extension of life expectancy. Patients frequently experience substantial relief from angina and an enhanced ability to engage in daily activities. However, it is imperative to understand that while CABG addresses the anatomical blockages, it does not cure the underlying atherosclerosis. Therefore, a lifelong commitment to a heart-healthy lifestyle is essential. This includes adhering to a balanced diet, maintaining regular physical activity, abstaining from smoking, and diligently managing conditions such as high blood pressure, high cholesterol, and diabetes. Regular follow-up with a cardiologist is crucial to monitor the patency of the grafts and the overall cardiac health, ensuring the sustained benefits of this critical procedure.


{kind=link}