This comprehensive diagram illustrates the various configurations of Coronary Artery Bypass Graft (CABG) surgery, ranging from single to quadruple bypasses. Each panel visually demonstrates how different numbers of grafts are used to circumvent blockages in the coronary arteries, depending on the extent of coronary artery disease. Understanding these distinctions is crucial for appreciating the individualized approach taken in treating patients with varying degrees of arterial obstruction and for comprehending the profound impact of this surgical intervention on cardiac blood flow.
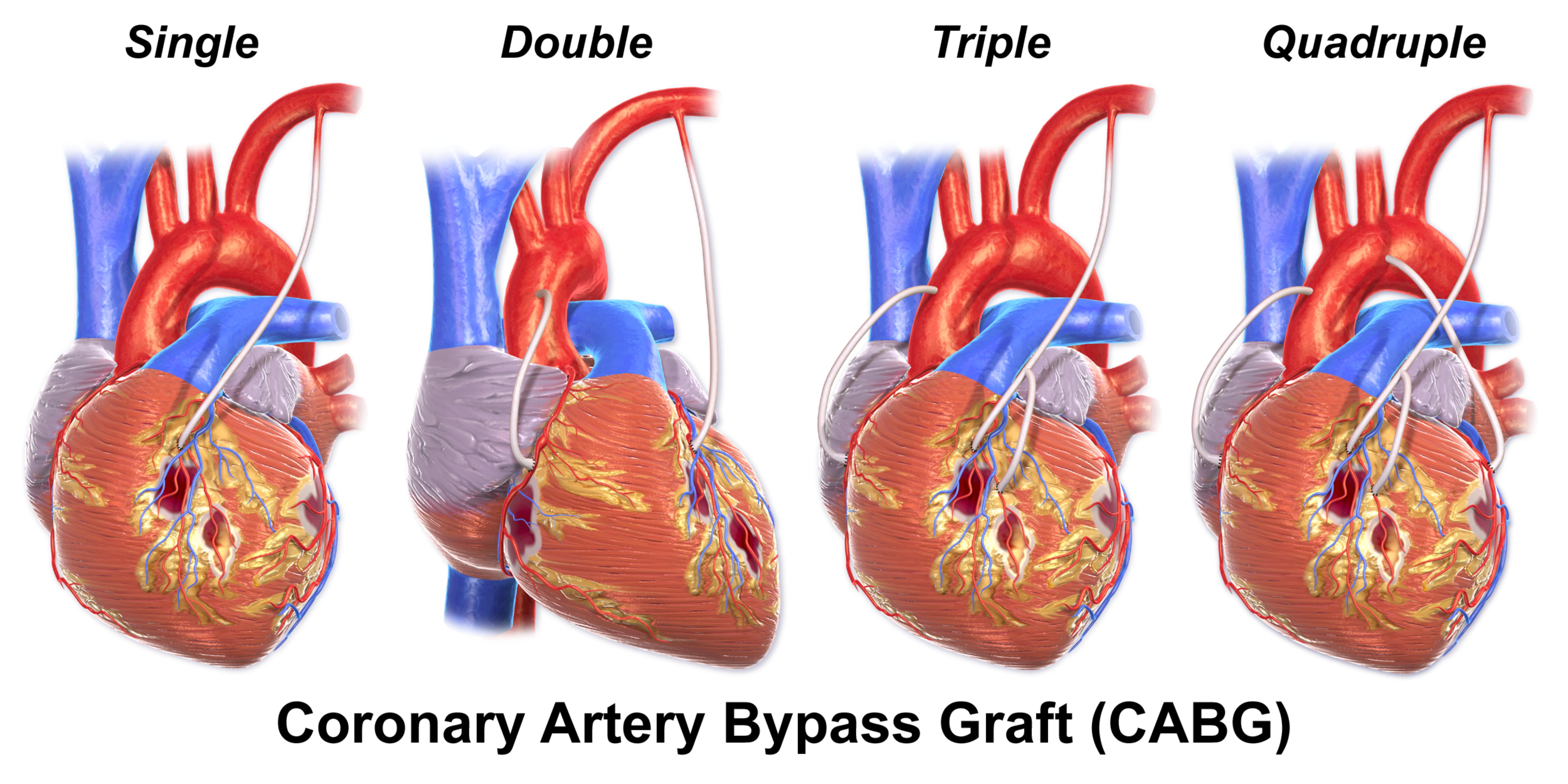
Single: This panel depicts a single bypass graft being implemented to restore blood flow to one blocked coronary artery. This approach is typically used when only one major coronary artery has a significant blockage requiring surgical intervention. The graft creates a new path for blood to flow around the single obstruction.
Double: The “Double” panel shows two bypass grafts used to revascularize two distinct blocked coronary arteries. This procedure addresses multiple areas of significant narrowing, ensuring improved blood supply to two different regions of the heart muscle. Each graft is strategically placed to bypass an individual obstruction.
Triple: In the “Triple” configuration, three separate bypass grafts are utilized to bypass three different blocked coronary arteries. This indicates a more extensive form of coronary artery disease, affecting multiple vital vessels supplying the heart. The triple bypass significantly enhances overall cardiac perfusion.
Quadruple: The “Quadruple” panel illustrates the most extensive form shown, with four bypass grafts created to overcome blockages in four different coronary arteries. This procedure is reserved for patients with severe, widespread coronary artery disease, where multiple crucial vessels are significantly obstructed. A quadruple bypass offers comprehensive revascularization for extensively compromised cardiac blood flow.
Introduction to Coronary Artery Bypass Graft (CABG) Options
Coronary Artery Bypass Graft (CABG) surgery is a cornerstone treatment for advanced coronary artery disease (CAD), a condition characterized by the narrowing or blockage of the heart’s arteries due to plaque buildup. When these blockages impede adequate blood flow to the myocardium (heart muscle), patients can experience debilitating symptoms such as angina, shortness of breath, and face a high risk of myocardial infarction (heart attack). CABG surgery addresses this by creating new pathways for blood to flow around the obstructed segments, thereby restoring oxygen and nutrient supply to the heart. The provided diagram effectively illustrates the different complexities of CABG, from a single bypass to a quadruple bypass, reflecting the varying extent of disease.
The number of bypasses performed (single, double, triple, or quadruple) directly corresponds to the number of major coronary arteries that require revascularization. This tailored approach ensures that each significant blockage is addressed, optimizing blood flow to all affected areas of the heart. The decision on how many bypasses are needed is made by a cardiac surgery team after a thorough diagnostic evaluation, including coronary angiography, which maps out the exact locations and severity of arterial blockages. This personalized strategy is critical for achieving the best possible surgical outcomes and improving the patient’s long-term cardiac health.
CABG surgery involves harvesting healthy blood vessels, typically from the patient’s leg (saphenous vein) or chest (internal mammary artery), to serve as grafts. These grafts are then meticulously sewn onto the coronary arteries, bypassing the diseased segments. The procedure fundamentally aims to improve the quality of life by alleviating symptoms, enhancing cardiac function, and potentially extending life expectancy.
Key considerations guiding the number of bypasses in CABG include:
- Number of significantly stenosed coronary arteries: Each major artery with a critical blockage typically receives a bypass.
- Severity of blockages: Only hemodynamically significant blockages (those severely impeding blood flow) are bypassed.
- Location of blockages: Critical areas like the left main coronary artery or proximal LAD often necessitate bypassing.
- Patient’s overall health and comorbidities: Influences the surgical plan and risk assessment.
- Quality and availability of graft vessels: Determines how many suitable bypass conduits can be harvested.
- Long-term patency of different graft types: Internal mammary artery grafts typically have superior long-term patency compared to saphenous vein grafts.
These factors are carefully weighed by the surgical team to determine the most effective revascularization strategy.
The Anatomy of Coronary Arteries and CAD Progression
The heart is supplied with oxygenated blood by two main coronary arteries: the left main coronary artery (LMCA) and the right coronary artery (RCA). The LMCA typically branches into the left anterior descending (LAD) artery and the circumflex artery (LCx). The LAD supplies the front and bottom of the left ventricle and the anterior two-thirds of the interventricular septum, making it a crucial vessel. The LCx wraps around the left side of the heart, supplying the left atrium and the posterior wall of the left ventricle. The RCA, originating from the right side, typically supplies the right atrium, right ventricle, and in most individuals, the inferior wall of the left ventricle and the posterior one-third of the interventricular septum.
Coronary artery disease (CAD) develops when atherosclerotic plaque accumulates within these arteries, causing them to narrow and harden. This progressive disease can affect one, two, three, or even all four major coronary arteries or their significant branches. The number of affected arteries is a key determinant in classifying the extent of CAD (e.g., single-vessel disease, multi-vessel disease). As the disease progresses, the heart muscle downstream from the blockage receives insufficient oxygen, leading to ischemia. If left untreated, this can result in chronic angina, heart attacks, and heart failure. The necessity for single, double, triple, or quadruple bypasses directly reflects the widespread nature and severity of these arterial obstructions across the heart’s vascular network.
Surgical Techniques for Different Bypass Configurations
The fundamental principle of CABG remains consistent across single to quadruple bypasses: creating new conduits for blood flow around arterial blockages. The primary difference lies in the number of grafts implanted and the specific coronary arteries targeted.
- Single Bypass: Addresses a single critical blockage, often in a major vessel like the LAD. A common approach is to use the left internal mammary artery (LIMA) to bypass the LAD, known for its excellent long-term patency.
- Double Bypass: Involves bypassing two distinct blocked arteries. This might include the LIMA to LAD, combined with a saphenous vein graft (SVG) to another artery, such as the right coronary artery (RCA) or a branch of the circumflex artery.
- Triple Bypass: Three grafts are utilized for three separate blockages. A typical configuration could be LIMA to LAD, an SVG to the RCA, and another SVG to a circumflex marginal branch. This addresses more extensive multi-vessel disease.
- Quadruple Bypass: The most extensive form shown, addressing four significant blockages. This requires careful planning to select appropriate graft vessels and meticulously connect them to four different coronary arteries or their major branches. Given the number of grafts, a combination of IMA and SVG conduits is typically used.
Each bypass connection (anastomosis) is meticulously performed by the cardiac surgeon. The ability to perform multiple bypasses in a single operation underscores the precision and complexity of modern cardiac surgery, allowing for comprehensive revascularization and significantly improving myocardial perfusion.
Recovery and Long-Term Outcomes Post-CABG
Regardless of the number of bypasses performed, the recovery process after CABG surgery is comprehensive. Patients typically spend several days in intensive care for close monitoring, followed by a stay in a regular hospital ward. Pain management, wound care for the chest incision and graft harvest sites, and gradual mobilization are key components of immediate post-operative care. Cardiac rehabilitation programs are crucial for long-term recovery, focusing on supervised exercise, dietary modifications, and education on managing cardiovascular risk factors.
The long-term outcomes for patients undergoing CABG, especially those with multi-vessel disease, are generally very positive. Studies have shown significant improvements in symptoms, quality of life, and survival rates compared to medical therapy alone in specific patient populations. However, it is vital for patients to understand that CABG is a treatment for the effects of atherosclerosis, not a cure for the disease itself. Therefore, strict adherence to a heart-healthy lifestyle, including a balanced diet, regular physical activity, smoking cessation, and meticulous management of conditions like hypertension, diabetes, and dyslipidemia, is paramount. Regular follow-up with a cardiologist is essential to monitor the patency of the grafts and the overall cardiac health, ensuring the benefits of the surgery are sustained over time.


{kind=link}