Introduction to Thoracic Imaging in Adolescents
Chest X-rays are foundational diagnostic tools for evaluating respiratory conditions across all age groups. In adolescents, interpreting these images requires consideration of their unique physiological characteristics and potential comorbidities. This article will present a case study of a 15-year-old male with a complex medical history, focusing on the interpretation of his chest X-ray, associated clinical findings, and initial management.
Clinical Presentation
The patient is a 15-year-old male with a history of chronic Idiopathic Thrombocytopenic Purpura (ITP) and asthma. He regularly uses montelukast 10mg once daily orally in the evening, budesonide nasal spray once daily (with additional doses if he experiences respiratory tightness), and mometasone furoate nasal spray once daily in the evening.
He presented with a history of sore throat, postnasal drip, cough, and dyspnea, which began approximately 10 days prior. One week ago, he visited the emergency department where he was prescribed ceftriaxone (proper doses intramuscularly) for 3 days and advised to follow up. A repeat chest X-ray showed no change in the affected areas, leading to a prescription of clarithromycin and cefuroxime. He was asked to return for a follow-up on Monday. His symptoms persisted, and he developed chest pain today.
Current Presentation and Further Investigations:
- Today’s Visit: Persistent symptoms with new onset chest pain.
- Computed Tomography (CT) Scan of Thorax Result: “Ground-glass opacities and peribronchial infiltration observed in the right upper lobe.”
- Past Medical History: Approximately 10 days of ward admission due to COVID-19 in the past. Fully vaccinated.
- Symptoms: No fever, no weight loss. Reports night and day sweats. No family history of tuberculosis.
- Past Diagnoses:
- Diagnosed with ITP at 5 months of age, followed up at Çapa (Istanbul University Cerrahpaşa Faculty of Medicine), with controls every 6 months.
- Diagnosed with allergic asthma 2 years ago at Çam and Sakura City Hospital, regularly using montelukast, budesonide, and mometasone.
The patient was admitted to the ward with preliminary diagnoses of tuberculosis and pneumonia.
Physical Examination Findings (Day 1 of Hospitalization):
- General Condition: Moderate, vital signs stable.
- Skin: Natural, no rashes observed.
- Head and Neck: Normal.
- Oropharynx: Hyperemic.
- Respiratory System: Exhibits coarse inspiratory and expiratory rhonchi and crackles, monitored in room air.
- Cardiovascular System: Normal heart sounds (S1, S2) with no additional sounds or murmurs. Peripheral pulses are palpable bilaterally.
- Gastrointestinal System: Abdomen is soft, non-tender, with no defense or rebound tenderness. Bowel sounds present, with normal gas and stool passage.
- Genitourinary System: Male external genitalia, no major urogenital anomaly, with adequate urine output.
- Neuromuscular System: Glasgow Coma Scale (GCS) of 15. Conscious, pupils are isochoric and reactive to light. Neuromotor development is appropriate for age. No signs of meningeal irritation.
- Extremities: Normal, no deformities.
- Current Complaints: Sore throat, postnasal drip, cough are present, no additional complaints.
Radiological Findings: Chest X-ray
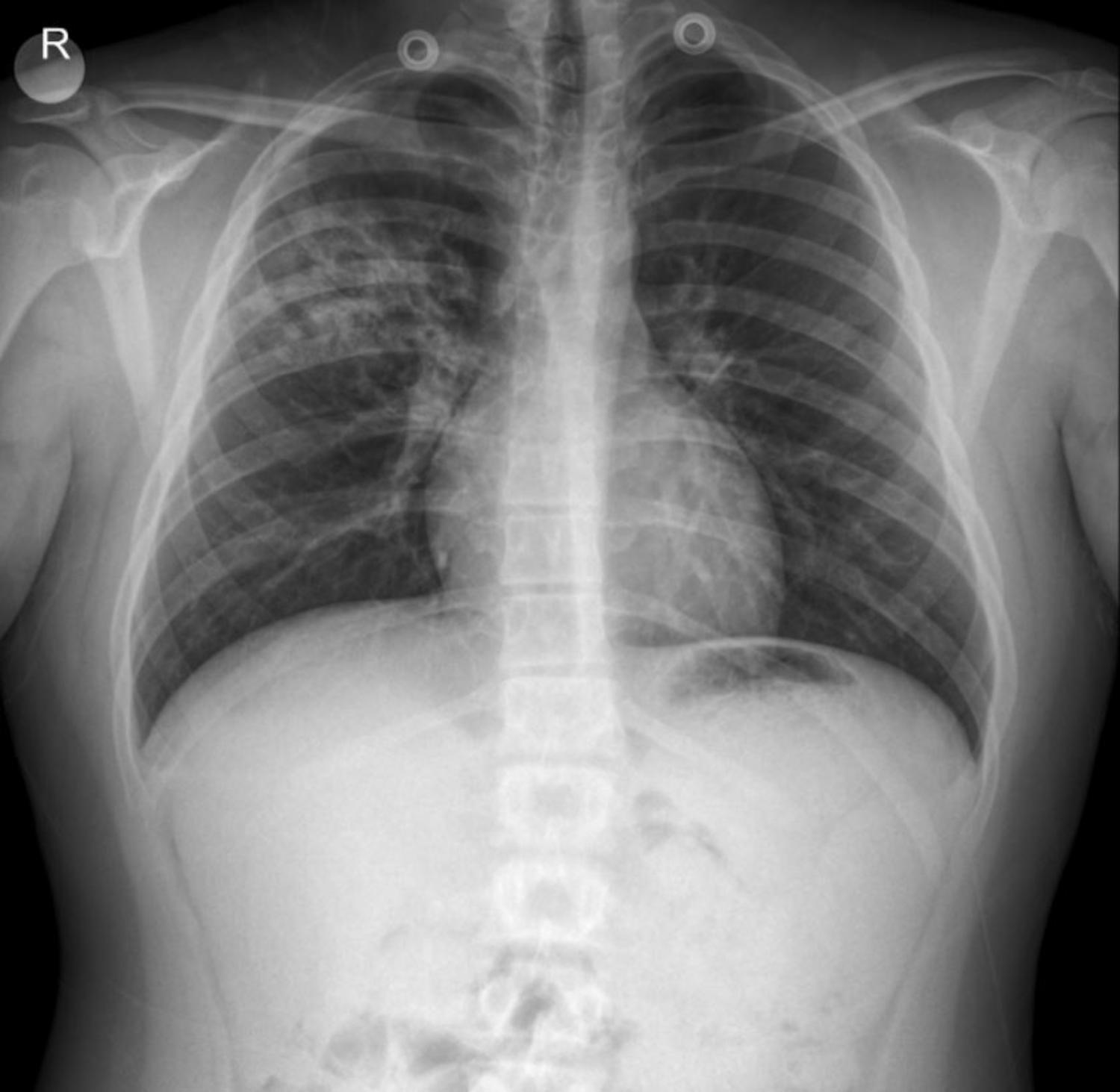
The provided anterior-posterior (AP) chest X-ray of the adolescent male reveals several key features:
- Lungs: The most prominent finding is a significant infiltration localized to the right upper and mid lobes. This appears as an area of increased opacity with heterogeneous density, suggesting consolidation and/or inflammatory changes. While the case notes indicate paracardial infiltration in previous discussions, in this specific image, the primary and most striking finding is the extensive infiltration in the right upper-mid lobe, with potential involvement extending toward the hilum. The CT report of “ground-glass opacities, peribronchial infiltration in the right upper lobe” correlates well with these X-ray findings. The left lung field appears relatively clear in comparison, though subtle peribronchial markings might be present.
- Heart: The cardiac silhouette appears within normal limits for size and contour.
- Diaphragm: The diaphragmatic contours are clear and sharp, with no evidence of pleural effusions.
- Bony Thorax: The ribs and clavicles appear intact, with no obvious fractures or deformities. The skeletal structures are appropriate for the patient’s age.
- Trachea: The trachea appears patent and centrally located.
- Medical Devices: Two circular radiopaque densities are noted superior to the lung fields, likely representing external medical devices or clothing artifacts.
Given the persistent respiratory symptoms, the history of previous antibiotic failures, and the significant localized infiltration seen on the X-ray (and confirmed by CT), along with systemic symptoms like night sweats, the differential diagnoses of pneumonia (including atypical pneumonia) and tuberculosis are highly relevant. The patient’s underlying asthma and history of ITP also complicate the clinical picture.
Management Plan (Day 1 of Hospitalization for Suspected Tuberculosis/Pneumonia)
The following plan is outlined for the patient:
- Laboratory Investigations:
- Fasting gastric fluid will be collected for 3 consecutive days starting tomorrow (after oral intake cessation after midnight).
- Sputum for Acid-Fast Bacilli (AFB) smear and culture will be sent if the patient can produce a sample.
- Serum Protein Electrophoresis (SPEP) will be sent tomorrow.
- PPD (Purified Protein Derivative) test is planned.
- Follow-up on previous blood culture results (dated 17.11).
- Antibiotic Therapy: Antibiotic regimen will be decided after consultation with the pediatric infectious disease department.
- General Care: Monitoring of general condition and vital signs.
Disclaimer: Drug types and dosages should always be confirmed with the relevant dosage guidelines in your country or by consulting a licensed physician in the department. This information is for educational purposes only.
Conclusion
This case illustrates the critical role of chest X-rays in the diagnostic pathway for adolescents presenting with persistent respiratory symptoms and complex medical histories. The prominent right upper-mid lobe infiltration seen on the X-ray, supported by CT findings, necessitates a comprehensive workup to differentiate between various infectious etiologies, particularly pneumonia and tuberculosis, especially in a patient with a history of recurrent respiratory issues and an immunocompromised state (due to chronic ITP management).
Please note: This content is intended for educational purposes and reference only. It should not be used as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of a qualified healthcare provider for any medical concerns.


{kind=link}