This article presents a compelling case study of a pediatric patient, emphasizing the critical role of chest radiography in diagnosing and managing common respiratory complaints in infants. We will analyze the provided chest X-ray in conjunction with the patient’s clinical presentation and management, offering insights relevant to medical students and practitioners.
Pediatric Pneumonia: A Chest X-ray Case Study for Medical Professionals
Patient Presentation
A 1-month-20-day-old female infant, born via C-section at 39 weeks with a birth weight of 3200g, presented to the emergency department with a 2-day history of rhinorrhea and fever. Her feeding significantly decreased on the day of admission. A family history revealed flu-like symptoms among other household members.
Initial Assessment and Findings
Upon evaluation, the infant exhibited:
- Elevated C-reactive protein (CRP): 30, indicating an inflammatory process.
- Peripheral Oxygen Saturation (SpO2): 90% on room air, necessitating oxygen support.
- Chest X-ray (PAAC): Revealed infiltrations.
Given these findings, an initial diagnosis of community-acquired pneumonia was suspected.
Management in the Emergency Department
The patient was promptly initiated on empirical antibiotic therapy:
- Cefotaxime: with proper doses
- Ampicillin-sulbactam: with proper doses
Additionally, due to low oxygen saturation, the patient was placed on a nebulizer mask. For further investigation and management, the infant was admitted to the pediatric ward.
Please consult your national guidelines for appropriate drug types and dosages, or seek advice from a qualified medical professional in the relevant department.
Clinical Course on the Pediatric Ward (Day 1)
On the first day of hospitalization, the patient’s condition showed some improvement:
- General Condition: Moderate, vital signs stable.
- Fever: Absent.
- Feeding: Good, strong suckling.
- Oxygen Saturation: Improved to 94-95% on room air, maintained with a nebulizer mask.
- Respiratory System: Natural, clear lung sounds on auscultation (no rales or rhonchi).
The antibiotic regimen of Cefotaxime and Ampicillin-sulbactam was continued with proper doses.
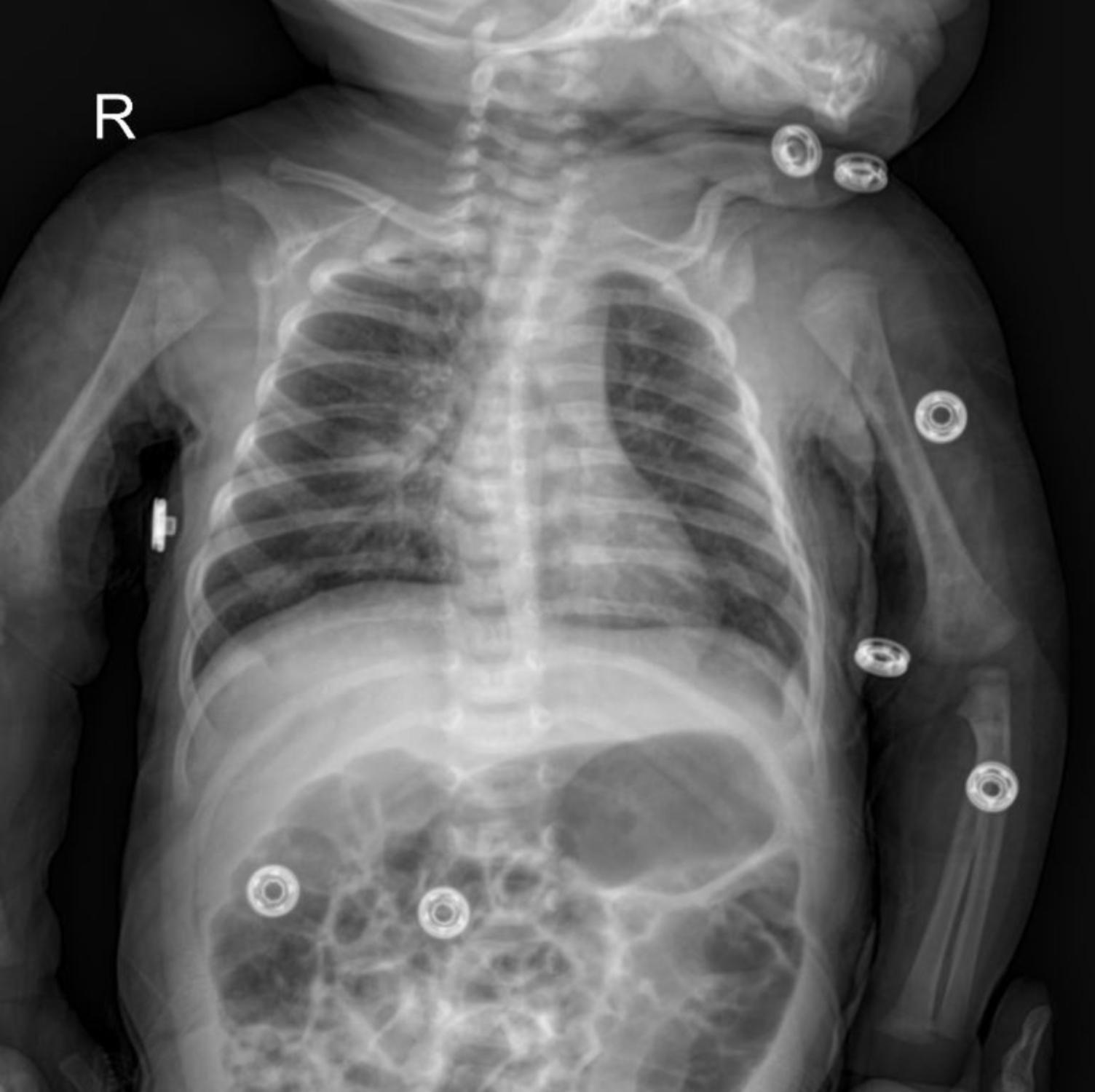
The image shows a frontal chest radiograph of an infant. Key features to observe include:
- Diffuse Bilateral Infiltrates: The most striking feature is the presence of widespread, ill-defined opacities throughout both lung fields. These infiltrates suggest an inflammatory process, consistent with pneumonia.
- Perihilar and Lower Lobe Consolidation: There appears to be denser consolidation, particularly around the hila and in the lower lobes. This indicates areas where the alveoli are filled with exudate, a classic sign of bacterial pneumonia.
- Small Right Pleural Effusion: A subtle blunting of the right costophrenic angle (highlighted by the blue circle) suggests a small pleural effusion, which can accompany pneumonia.
- Air Bronchograms: While not explicitly highlighted, careful inspection might reveal air bronchograms within consolidated areas, further supporting the diagnosis of pneumonia.
- Right-sided Marker “R”: Indicates the right side of the patient.
- Artifacts: The circular metallic objects seen on the patient’s shoulders and limbs are likely ECG leads or other monitoring devices, and should not be confused with pathology.
The combination of diffuse infiltrates, consolidation, and a small pleural effusion on the chest X-ray strongly supports the clinical suspicion of pneumonia in this infant.
Conclusion
This case effectively illustrates the typical presentation, radiological findings, and initial management of pneumonia in a young infant. The chest X-ray served as a crucial diagnostic tool, guiding the initiation of appropriate antibiotic therapy and ongoing respiratory support. The second case provides a valuable comparison, highlighting the variability in disease progression and the need for individualized patient management.
This content is intended for educational purposes only and should not be used as a basis for diagnosis or treatment. Always consult with a qualified healthcare professional for medical advice.


{kind=link}