The superior mediastinum is a critical anatomical crossroads where the major vascular pathways of the heart intersect with the primary structures of the neck and thoracic cavity. This guide explores the intricate relationships between the right and left common carotid arteries, the brachiocephalic vessels, and the surrounding neurovascular structures as viewed in a cadaveric dissection. Understanding these spatial arrangements is essential for clinical diagnosis, surgical planning, and the interpretation of cardiovascular imaging.
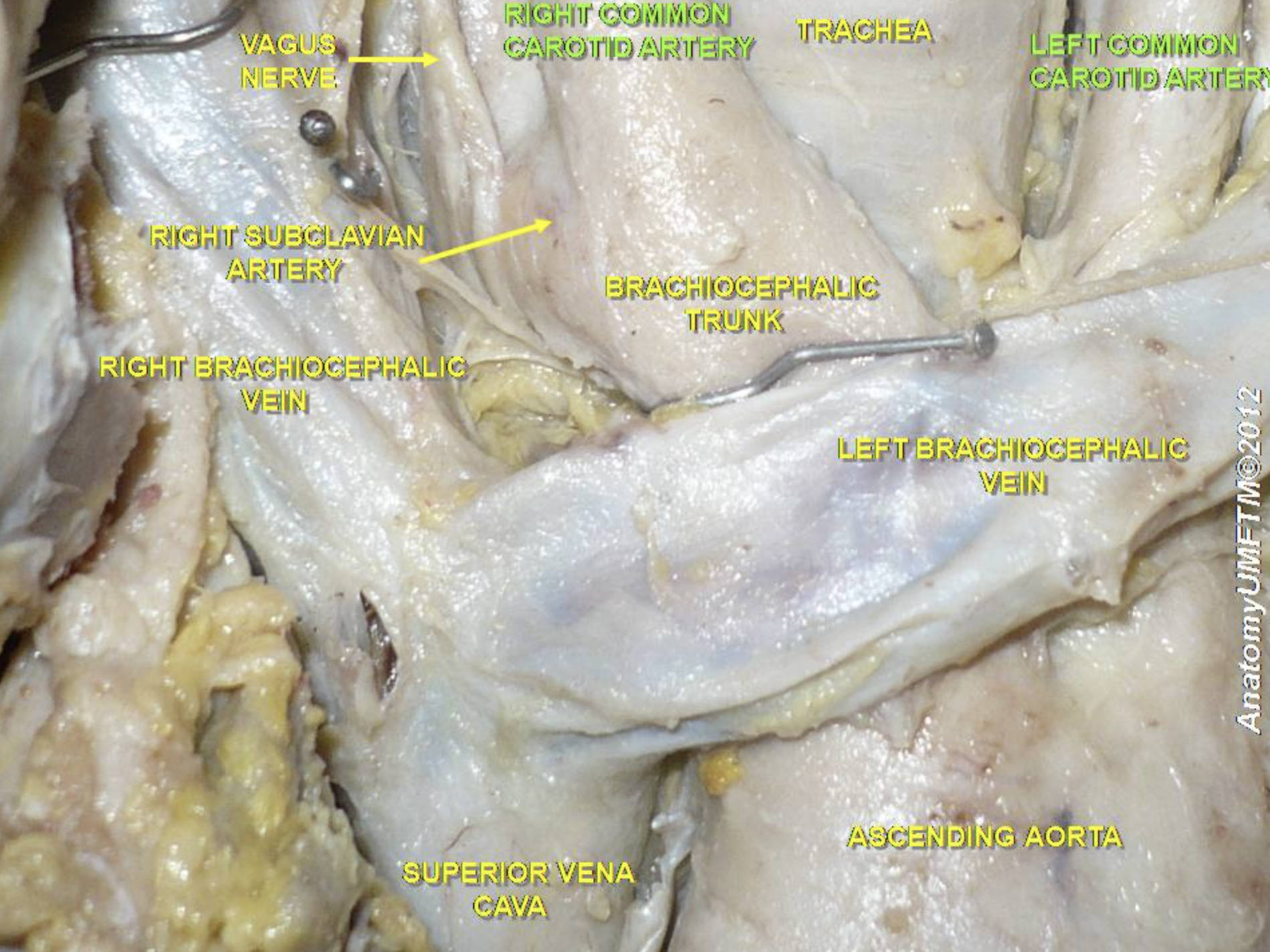
VAGUS NERVE: This is the tenth cranial nerve, which provides essential parasympathetic innervation to the thoracic and abdominal organs. In the superior mediastinum, it descends within the carotid sheath, typically positioned posterior to the common carotid artery and internal jugular vein.
RIGHT COMMON CAROTID ARTERY: This major vessel arises from the brachiocephalic trunk behind the right sternoclavicular joint. It ascends into the neck to supply oxygenated blood to the right hemisphere of the brain, the right eye, and various facial structures.
TRACHEA: The trachea is the midline airway tube reinforced by C-shaped cartilaginous rings that prevent its collapse during respiration. It sits posterior to the great vessels and anterior to the esophagus, serving as a primary landmark for identifying adjacent neurovascular structures.
LEFT COMMON CAROTID ARTERY: Unlike its counterpart on the right, this artery usually arises directly from the aortic arch as its second major branch. It ascends into the left side of the neck to provide the primary arterial supply for the left side of the head and neck.
RIGHT SUBCLAVIAN ARTERY: Originating from the brachiocephalic trunk, this artery courses laterally toward the right upper limb. It is responsible for supplying oxygenated blood to the right arm, shoulder, and segments of the thoracic wall.
BRACHIOCEPHALIC TRUNK: This is the first and largest branch of the aortic arch, often referred to as the innominate artery. It provides a common origin for the right common carotid and right subclavian arteries before they diverge to supply their respective territories.
RIGHT BRACHIOCEPHALIC VEIN: This vessel is formed by the union of the right internal jugular and right subclavian veins. It follows a relatively short and vertical course, joining with the left brachiocephalic vein to form the superior vena cava.
LEFT BRACHIOCEPHALIC VEIN: This vein is significantly longer than the right because it must cross the midline of the chest. It passes anterior to the major branches of the aortic arch, making it a critical structure to protect during midline thoracic surgical approaches.
SUPERIOR VENA CAVA: This large venous trunk is responsible for returning deoxygenated blood from the upper half of the body to the heart’s right atrium. It is approximately 7 centimeters long and is formed by the convergence of the two brachiocephalic veins.
ASCENDING AORTA: The ascending aorta is the first segment of the systemic circulatory circuit, emerging directly from the left ventricle. It carries the entire cardiac output and transitions into the aortic arch, where it gives off the primary vessels supplying the head and arms.
The Organization of the Thoracic Inlet
The thoracic inlet, or superior thoracic aperture, serves as the gateway between the neck and the thorax. Within this compact space, the mediastinal anatomy is organized with incredible efficiency to allow for the passage of the “great vessels,” nerves, and airways. The asymmetry between the right and left sides is one of the most striking features of this region; for instance, the left common carotid artery and left subclavian artery arise directly from the aortic arch, while their right-sided counterparts share a common origin in the brachiocephalic trunk.
Understanding these relationships is vital for managing clinical conditions such as Carotid Artery Disease (CAD). This pathology occurs when atherosclerotic plaque builds up in the arterial walls, leading to stenosis or narrowing of the vessel lumen. If left untreated, CAD significantly increases the risk of ischemic stroke, as plaque fragments or blood clots can embolize and travel to the brain. Diagnostic tools like carotid duplex ultrasound or CT angiography are frequently used to visualize the flow through these vessels and assess the degree of blockage.
Key anatomical considerations in this region include:
- The proximity of the vagus and phrenic nerves to the major venous and arterial trunks.
- The position of the trachea as a central anchor for the surrounding neurovascular bundles.
- The role of the brachiocephalic veins in facilitating venous return from the head and upper extremities.
- The high-pressure nature of the ascending aorta and its susceptibility to aneurysmal dilation.
Neurovascular Coordination and Hemodynamic Stability
The coordination between the nervous system and the vascular network in the superior mediastinum is essential for maintaining hemodynamic stability. The carotid sinus, located near the bifurcation of the common carotid artery, contains specialized baroreceptors that sense changes in arterial pressure. These sensors send signals via the glossopharyngeal nerve to the brainstem, which then utilizes the vagus nerve to adjust the heart rate and vascular resistance accordingly. This feedback loop ensures that the brain receives a constant supply of blood regardless of changes in posture or physical activity.
The aortic arch serves as the central hub for this distribution, branching into the vessels that will eventually form the Circle of Willis in the brain. Any congenital variations in the branching pattern of the arch, such as a “bovine arch,” can have significant implications for interventional procedures like carotid stenting or cardiac catheterization. Furthermore, the relationship between the trachea and the left brachiocephalic vein is a major consideration during tracheostomy; if the vein is positioned unusually high, it can be at risk of accidental injury during the procedure.
In conclusion, the anatomy of the common carotid arteries and the superior mediastinum is a masterclass in structural integration. From the parasympathetic signals of the vagus nerve to the high-volume transport of the superior vena cava, every component works in unison to support the body’s metabolic and respiratory needs. A thorough mastery of these cadaveric details allows medical professionals to navigate the complexities of human physiology with precision, ensuring safer surgical outcomes and more accurate clinical assessments.


{kind=link}