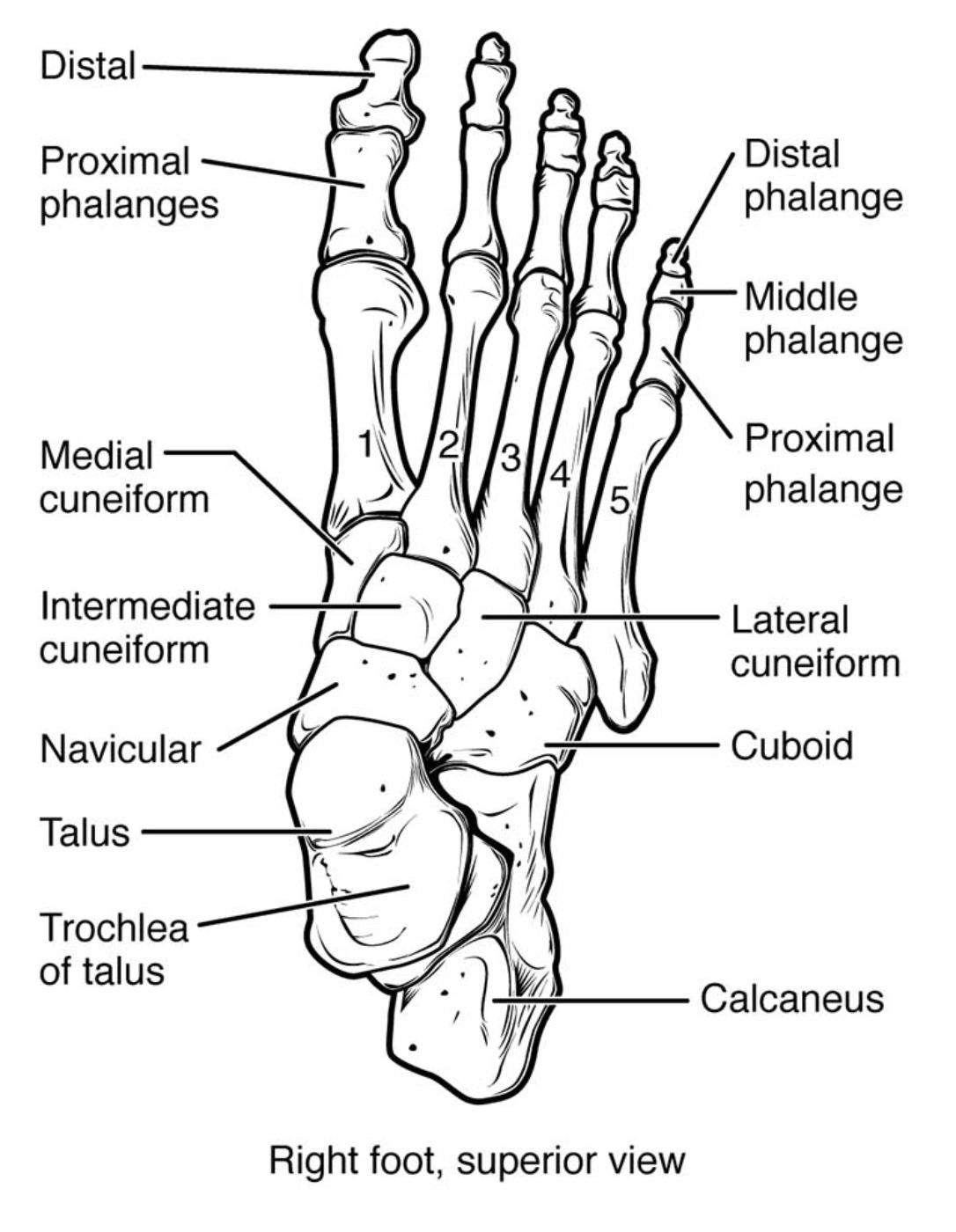
The human foot is a marvel of evolutionary engineering, comprising 26 bones, 33 joints, and over a hundred muscles, tendons, and ligaments. From a medical perspective, the foot must balance the competing demands of rigidity for propulsion and flexibility for shock absorption. This superior (dorsal) view of the right foot provides a clear anatomical map of the hindfoot, midfoot, and forefoot, which is essential for diagnosing common pathologies such as stress fractures, ligamentous tears, and degenerative joint disease.
Label-by-Label Explanation
Distal phalange
These are the bones at the tips of the toes. In the hallux (great toe), there is only one distal phalanx articulating with the proximal phalanx, whereas the four lateral toes have distal, middle, and proximal phalanges. These bones serve as attachment points for the flexor and extensor tendons, facilitating balance and grip during the gait cycle.
Middle phalange
The middle phalanges are found only in the second through fifth toes. They sit between the proximal and distal phalanges, providing additional segments for flexion and extension of the digits. Clinically, these are significant in conditions like hammer toe or claw toe, where muscular imbalances lead to fixed flexion at the interphalangeal joints.
Proximal phalange
These bones form the base of the toes and articulate with the metatarsal heads at the metatarsophalangeal (MTP) joints. They are the longest of the phalanges and play a critical role in weight distribution during the “toe-off” phase of walking. Injuries here often involve phalangeal fractures or MTP joint dislocations.
Metatarsals (1, 2, 3, 4, 5)
These five long bones constitute the midfoot-to-forefoot transition. The first metatarsal is the shortest and thickest, bearing significant weight, while the second metatarsal is the longest and most rigid, often prone to stress fractures in athletes. The base of the fifth metatarsal is a common site for avulsion or Jones fractures due to its relationship with the peroneus brevis tendon.
Medial cuneiform
The largest of the three cuneiform bones, it is situated on the medial aspect of the foot. It articulates with the navicular proximally and the first metatarsal distally, forming part of the medial longitudinal arch. It is a vital structural component for maintaining the arch’s height and resisting collapse during weight-bearing.
Intermediate cuneiform
This wedge-shaped bone is located between the medial and lateral cuneiforms. It articulates with the second metatarsal and is a key component of the transverse arch of the foot. Its relatively fixed position provides stability to the midfoot, serving as a cornerstone for the second metatarsal base.
Lateral cuneiform
Positioned in the center of the midfoot, the lateral cuneiform articulates with the third metatarsal, the intermediate cuneiform, the navicular, and the cuboid. This central location makes it an important link for distributing forces across the midtarsal region. It contributes to the overall structural integrity of the midfoot mortise.
Navicular
This boat-shaped bone is located on the medial side of the foot between the talus and the three cuneiforms. It is a critical landmark for the tibialis posterior tendon attachment. Clinically, the navicular is prone to stress fractures and is the primary bone involved in Koehler’s disease or accessory navicular syndrome.
Cuboid
The cuboid is located on the lateral side of the foot, articulating with the calcaneus proximally and the fourth and fifth metatarsals distally. It provides stability to the lateral column of the foot. Because it contains a groove for the peroneus longus tendon, it is functionally linked to the lateral stability and eversion of the foot.
Talus
The talus is a unique tarsal bone because it has no muscular attachments and is largely covered by articular cartilage. It connects the foot to the leg by articulating with the tibia and fibula at the ankle joint. It is responsible for transmitting the entire weight of the body from the leg to the foot.
Trochlea of talus
This is the superior, pulley-shaped articular surface of the talus that fits into the ankle mortise formed by the tibia and fibula. It is wider anteriorly than posteriorly, which explains why the ankle is more stable in dorsiflexion than in plantarflexion. Injuries to this surface, such as osteochondral lesions, can lead to chronic ankle pain and instability.
Calcaneus
The calcaneus, or heel bone, is the largest bone in the foot and the primary weight-bearing structure during the initial heel strike of the gait cycle. It serves as the insertion point for the Achilles tendon. Fractures of the calcaneus are often the result of high-energy axial loading, such as a fall from height, and can have a significant impact on long-term mobility.
Anatomical Overview
The bones of the foot are traditionally categorized into three functional regions: the hindfoot, midfoot, and forefoot. The hindfoot consists of the talus and calcaneus, which are responsible for early weight-bearing and ankle articulation. The midfoot includes the navicular, cuboid, and the three cuneiform bones, which act as a shock-absorbing bridge. Finally, the forefoot contains the metatarsals and phalanges, which provide the platform for balance and propulsion.
From the superior view, the complex articulations of the midfoot are visible, particularly the Lisfranc joint complex (tarsometatarsal joints). This region is structurally reinforced by strong ligaments but remains vulnerable to rotational and high-impact injuries. The spatial arrangement shown demonstrates how the cuneiforms and cuboid form a transverse arch that protects neurovascular structures on the plantar surface.
Functional Significance
The anatomical arrangement of the foot bones allows for the formation of three primary arches: the medial longitudinal, lateral longitudinal, and transverse arches. These arches are maintained by the shape of the bones (like the wedge-shaped cuneiforms), strong ligaments (such as the long plantar ligament), and the plantar fascia. The talus acts as the “keystone” of the medial longitudinal arch, receiving and distributing weight both posteriorly to the calcaneus and anteriorly through the midfoot.
During the gait cycle, the foot transitions from a flexible structure (pronated) to a rigid lever (supinated). The interaction between the tarsal bones at the midtarsal joint (Chopart’s joint) is essential for this transition. Without this osseous and ligamentous synchronization, the foot would be unable to adapt to uneven terrain or provide the necessary force for efficient movement.
Clinical Relevance
Understanding foot bone anatomy is vital for several clinical applications:
- Lisfranc Injuries: Damage to the tarsometatarsal joints often involves a separation between the second metatarsal base and the medial cuneiform, which can lead to long-term midfoot collapse.
- Hallux Valgus: Commonly known as a bunion, this involves a lateral deviation of the great toe and a medial prominence of the first metatarsal head.
- Fractures: The base of the 5th metatarsal and the neck of the talus are critical fracture sites that require careful monitoring due to potential blood supply issues (avascular necrosis).
- Diabetic Foot: Structural changes such as Charcot arthropathy can lead to the fragmentation of midfoot bones, significantly altering the foot’s shape and increasing ulcer risk.
For medical learners, mastering the foot’s anatomy requires a clear understanding of bone names, their relative positions, and their articulations. Being able to identify these structures on an X-ray or during a physical exam allows for more precise diagnostic reasoning. This superior view is particularly useful for learning the “tarsal row” and understanding how the midfoot bridges the stability of the hindfoot with the mobility of the forefoot.
Medical Learning Tips
- The hallux only has two phalanges, distal and proximal, whereas the other four toes have three.
- The talus is unique because it lacks any muscular attachments, relying entirely on ligamentous support.
- The second metatarsal base is firmly wedged between the medial and lateral cuneiforms, making it the most stable part of the midfoot.


{kind=link}