A robust term newborn weighing 4300 grams develops respiratory distress soon after uncomplicated vaginal delivery. Chest X-ray performed within one hour reveals a significant left-sided pneumothorax with lung collapse. Following urgent chest drain insertion, the follow-up radiograph confirms successful resolution and lung re-expansion. This newborn pneumothorax X-ray case emphasizes the need for rapid diagnosis and intervention in neonatal air leak syndromes to prevent deterioration in otherwise healthy term infants.
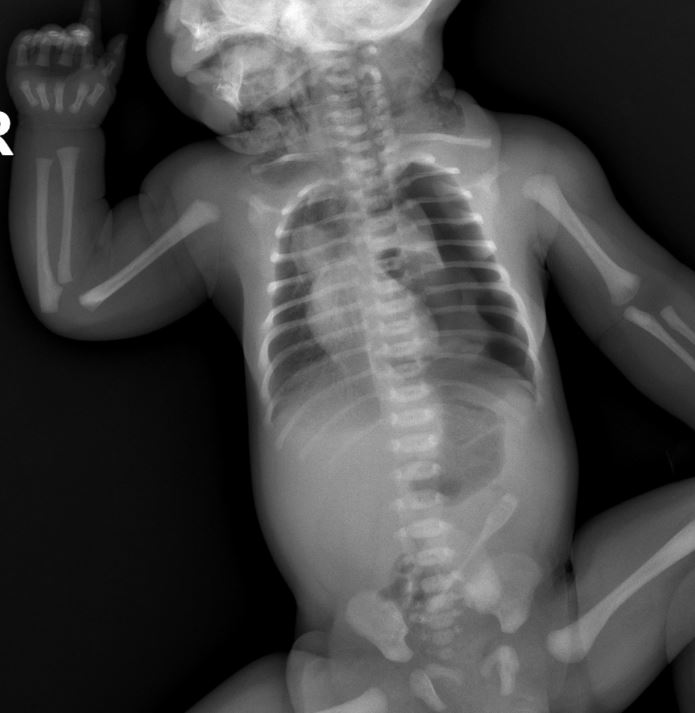
Left Hemithorax Hyperlucency The initial radiograph demonstrates increased radiolucency over the left chest compared to the right side, caused by free air in the pleural cavity. This lack of normal pulmonary vascular markings is a hallmark sign indicating the presence of pneumothorax in the newborn.
Collapsed Left Lung The left lung appears markedly compressed and retracted medially, with a visible visceral pleural line separating the collapsed lung from the surrounding free air. This collapse results from loss of negative intrapleural pressure, leading to impaired gas exchange and respiratory distress.
Mediastinal Shift to the Right The cardiac silhouette and mediastinal structures show deviation toward the right side due to pressure from the left pneumothorax. In tension pneumothorax, this shift can impair venous return, making prompt recognition and treatment essential.

Chest Drain Tube in Left Chest The post-insertion X-ray clearly shows the radiopaque chest drain positioned within the left hemithorax, typically inserted in the anterior or mid-axillary line. The tube facilitates evacuation of trapped air, allowing the lung to re-expand against the chest wall.
Re-expanded Left Lung Fields After chest drain placement, the left lung demonstrates improved aeration with restoration of normal lung markings and volume. The previously hyperlucent left hemithorax now matches the right side more closely, confirming effective resolution of the pneumothorax.
Normalized Mediastinal Position The heart and mediastinum return to a more central position following successful drainage. This indicates relief of tension and improved cardiopulmonary stability in the neonate.
Newborn pneumothorax is a potentially serious air leak condition that can occur even after normal vaginal birth in term infants. In this case involving a 4300-gram baby, respiratory distress prompted early imaging that identified left-sided pneumothorax with significant lung collapse. Chest drain insertion on the affected left side led to rapid healing, as evidenced by the follow-up X-ray showing re-expansion. Understanding the radiographic signs is crucial for neonatologists and pediatricians managing similar presentations.
What Causes Neonatal Pneumothorax?
Pneumothorax in newborns often arises from alveolar rupture due to high transpulmonary pressures during the initial breaths or crying. Air then dissects into the pleural space. Although more frequent in preterm infants or those requiring mechanical ventilation, spontaneous cases in large term babies like this 4300-gram infant can occur without obvious risk factors. Other contributors include transient tachypnea of the newborn, meconium aspiration, or vigorous resuscitation efforts.
Clinical Signs and When to Suspect Left-Sided Pneumothorax
Symptomatic neonates typically exhibit tachypnea, grunting, retractions, cyanosis, and asymmetric chest movement. Decreased breath sounds and hyperresonance are noted on the affected (left) side. In tension cases, hypotension or bradycardia may develop. Early chest X-ray is vital when respiratory distress appears shortly after birth, as in this case, to differentiate from other causes such as congenital diaphragmatic hernia or pneumonia.
Radiographic Features on Newborn Chest X-Ray
Key findings include unilateral hyperlucency without lung markings, a sharp pleural line outlining the collapsed lung, and contralateral mediastinal shift. In supine neonates, air may collect anteriorly, sometimes requiring additional views for confirmation. The initial image here shows classic left pneumothorax features with collapsed left lung, while the second image post-drainage demonstrates the chest tube in the left chest and healed, re-expanded lung fields.
Treatment with Chest Drain Insertion
Small asymptomatic pneumothoraces may resolve with observation or oxygen therapy. Symptomatic or tension pneumothorax requires immediate intervention. Needle aspiration can provide temporary relief, but definitive management usually involves chest tube (drain) insertion into the affected side—in this case, the left chest. The tube is connected to an underwater seal system to continuously remove air. Post-procedure X-ray verifies tube position and lung re-expansion, as seen in the healed image.
Potential Complications and Monitoring
Complications of untreated tension pneumothorax include cardiovascular compromise. Chest drain risks include infection, malposition (particularly on the left side near the heart), or bleeding. Close monitoring of vital signs, oxygen saturation, and serial radiographs ensures resolution. In this term infant, the rapid improvement after left-sided chest drain highlights the effectiveness of timely management.
Prognosis and Prevention in Neonatal Care
Most newborns with isolated pneumothorax recover fully once the air leak is resolved. Long-term outcomes are excellent when there is no underlying lung disease. Preventive measures focus on gentle delivery room resuscitation, minimizing barotrauma in ventilated infants, and maintaining high clinical suspicion for air leaks in any neonate with sudden respiratory distress. Education on radiographic interpretation improves early detection.
This detailed newborn pneumothorax X-ray case of left-sided involvement after normal vaginal birth serves as an educational resource for medical professionals. Prompt recognition of the collapsed left lung on initial imaging, followed by targeted chest drain insertion on the left side, resulted in complete healing. Such cases underscore the importance of preparedness in neonatal units for managing air leak syndromes effectively.


{kind=link}