When people hear the word ringworm, many immediately envision a parasitic worm burrowing under the skin. However, despite its misleading name, this condition is purely fungal. It is a highly contagious skin infection caused by mold-like parasites that live on the cells in the outer layer of your skin. Because it presents as a circular, ring-like rash, the name stuck through the centuries. Understanding how this infection manifests across different skin tones is vital for early diagnosis and treatment, as the visual cues can vary significantly depending on the amount of melanin in the skin. This guide explores the complexities of the infection, providing a deep dive into its appearance, causes, and the medical steps necessary to clear it up.
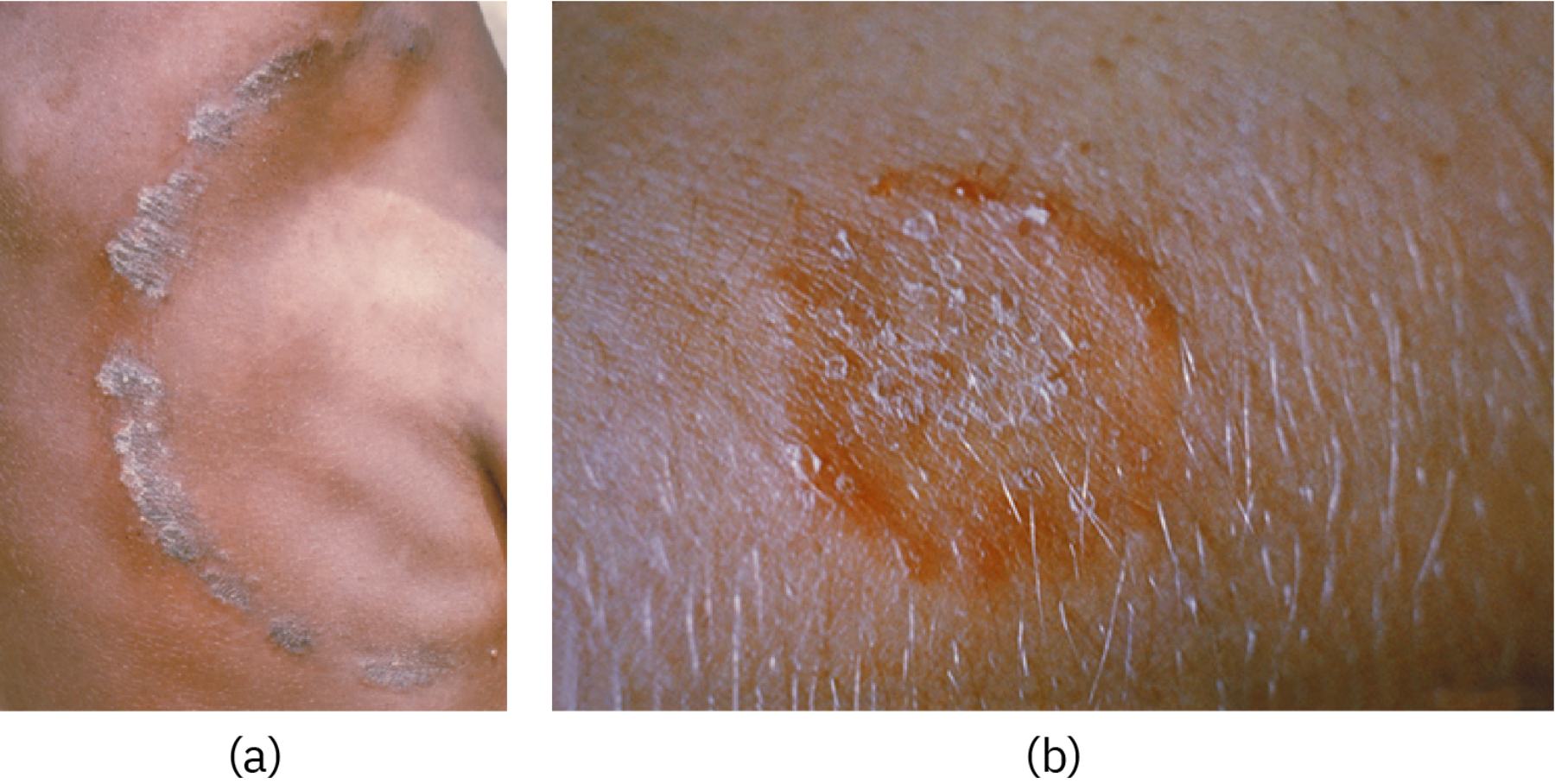
(a) This image shows the infection on brown or black skin, where the lesion often appears as a raised, scaly ring that is gray or brown. Unlike on lighter skin, the inflammatory response in melanated skin typically results in hyperpigmentation or a duller, grayish hue rather than bright red.
(b) This image displays the infection on lighter skin tones, characterized by a prominent, itchy, red circular rash with a clearer center. The contrast between the red, inflamed border and the surrounding healthy skin makes it the classic presentation most commonly associated with the condition in clinical textbooks.
The Biological Underpinnings of Tinea Corporis
Clinically referred to as tinea corporis, this infection is part of a larger family of fungal diseases. These infections are caused by dermatophytes, a specific group of fungi that require keratin—a protein found in skin, hair, and nails—to survive and reproduce. Because dermatophytes cannot penetrate deeper into the body, they remain localized on the surface, creating the characteristic circular patches we see. The fungus spreads outward in a radial fashion, which is why the edges of the rash are often the most inflamed and active, while the center may begin to heal or appear less irritated, creating the “ring” effect.
There are several types of dermatophytes responsible for these skin changes, primarily from the genera Trichophyton, Microsporum, and Epidermophyton. These organisms thrive in warm, moist environments, making certain areas of the body more susceptible than others. While the term tinea corporis refers specifically to the trunk, arms, and legs, the same fungus can affect the scalp (tinea capitis), the feet (tinea pedis, or athlete’s foot), and the groin (tinea cruris, or jock itch). Understanding that these are all variations of the same underlying fungal process helps patients realize that an infection in one area can easily spread to another through simple touch or shared towels.
Recognizing Symptoms Across Different Skin Tones
One of the most significant challenges in dermatology is the variation in how inflammatory conditions present on different skin phototypes. In patients with lighter skin, the most obvious sign is a red, scaly patch or bump that slowly expands. As it grows, the center often clears, leaving a scaly, red ring. The border is usually raised and may contain tiny blisters or pustules in more severe cases. The itching can be intense, leading to secondary bacterial infections if the skin is broken by scratching.
For individuals with darker skin tones (brown or black skin), the redness may be absent or very subtle. Instead, the ring may appear darker than the surrounding skin (hyperpigmented) or significantly lighter (hypopigmented) once the initial inflammation subsides. The texture is often a more reliable indicator than color; the border will feel slightly elevated and rough to the touch. In many cases, the rash might look more like a dry, ashy patch that doesn’t respond to standard moisturizers. Recognizing these nuances is essential for healthcare providers to avoid misdiagnosing the condition as eczema or psoriasis, which may require different treatment approaches.
How the Infection Spreads and Common Risk Factors
This fungal infection is notoriously easy to transmit. It spreads through four primary routes: human-to-human, animal-to-human, object-to-human, and rarely, soil-to-human. Direct skin-to-skin contact with an infected person is the most common method. However, many people are surprised to learn that they can contract it from their pets. Cats and dogs are frequent carriers, often showing patches of missing fur where the fungus is active. Handling an infected animal without washing your hands afterward is a quick way to develop a lesion on your arm or torso.
Environmental factors also play a massive role. Fungi love heat and humidity. This is why athletes, particularly wrestlers and those in contact sports, are at a higher risk. Shared locker rooms, gym mats, and damp towels are breeding grounds for dermatophytes. Furthermore, individuals with weakened immune systems or those who live in crowded living conditions are more likely to experience persistent or recurring infections. Maintaining a dry skin environment and practicing rigorous hygiene after visiting public fitness centers are the best defenses against environmental exposure.
Diagnostic Procedures in a Clinical Setting
While many cases are diagnosed by simple visual inspection, doctors sometimes need to confirm the presence of fungi to rule out other skin conditions. The most common diagnostic tool is a KOH (potassium hydroxide) prep test. A clinician gently scrapes a small amount of skin from the active border of the lesion and places it on a slide with KOH solution. Under a microscope, the KOH dissolves the skin cells but leaves the fungal hyphae (branching structures) visible, providing a definitive diagnosis.
In other instances, a Wood’s lamp—which uses ultraviolet light—might be used. Certain types of fungi will fluoresce or glow under this light, although this is not effective for all species of dermatophytes. If an infection is particularly stubborn or deep-seated, a fungal culture might be taken, where the sample is grown in a lab over several days or weeks to identify the specific species. This level of detail is usually reserved for cases that do not respond to initial rounds of standard therapy.
Effective Treatment Strategies
The primary method for clearing the infection involves the use of antifungal medications. Most localized cases on the body respond well to over-the-counter (OTC) topical creams, ointments, or powders. These products usually contain active ingredients like clotrimazole, miconazole, or terbinafine. It is crucial for patients to apply the medication not just to the visible ring, but also to a small area of healthy skin surrounding it, and to continue the treatment for the full duration recommended (usually two to four weeks), even if the rash disappears within the first few days.
For more extensive infections, or those involving the hair follicles or nails, topical treatments may not be enough. In these scenarios, a physician will prescribe oral antifungal pills. Oral medications like terbinafine or itraconazole work from the inside out, reaching the fungus through the bloodstream. These medications require a prescription and may necessitate blood tests to monitor liver function if taken over a long period. Regardless of the form of medicine, keeping the affected area clean and dry is a non-negotiable part of the healing process.
Prevention and Long-term Management
Preventing a recurrence requires a combination of personal hygiene and environmental awareness. Since the fungus can live on surfaces for extended periods, it is important to disinfect common areas if someone in the household is infected. Bedding, towels, and clothing should be washed in hot water and dried on a high-heat setting to kill any remaining spores. It is also wise to avoid sharing personal items like hairbrushes, razors, or unwashed gym clothes.
For pet owners, regular veterinary check-ups are essential. If you notice your pet scratching excessively or developing bald spots, seek veterinary care immediately to prevent the fungus from jumping to human family members. In public spaces like swimming pools or gym showers, always wear waterproof shoes or flip-flops to prevent the fungi from colonizing your feet and eventually spreading to the rest of your body. By staying vigilant and maintaining a dry, clean skin environment, most people can successfully avoid the discomfort and social stigma associated with these common fungal rashes.
When to Seek Professional Medical Advice
While many people successfully treat minor fungal infections at home, there are times when professional intervention is necessary. You should see a doctor if the rash does not improve after two weeks of consistent OTC treatment, or if the infection begins to spread rapidly to other parts of the body. Signs of a secondary bacterial infection—such as increased pain, swelling, warmth, or the presence of pus—require immediate medical attention and potentially a course of antibiotics.
Additionally, those with underlying health conditions like diabetes or HIV should consult a healthcare provider at the first sign of any skin infection. In these individuals, a simple fungal rash can quickly escalate into a more serious systemic issue if not managed correctly. A dermatologist can provide a tailored treatment plan that addresses the specific fungal strain and ensures that the skin barrier is restored effectively without leaving long-term scars or pigment changes.


{kind=link}