The arterial switch operation is a complex, life-saving open-heart surgery performed primarily on newborns to correct a critical congenital heart defect known as Transposition of the Great Arteries (TGA). In this condition, the two main arteries leaving the heart are reversed, preventing oxygenated blood from circulating to the body. This article analyzes the anatomical transformation achieved through this procedure, detailing the physiological correction from a parallel circulation to a normal series circulation.
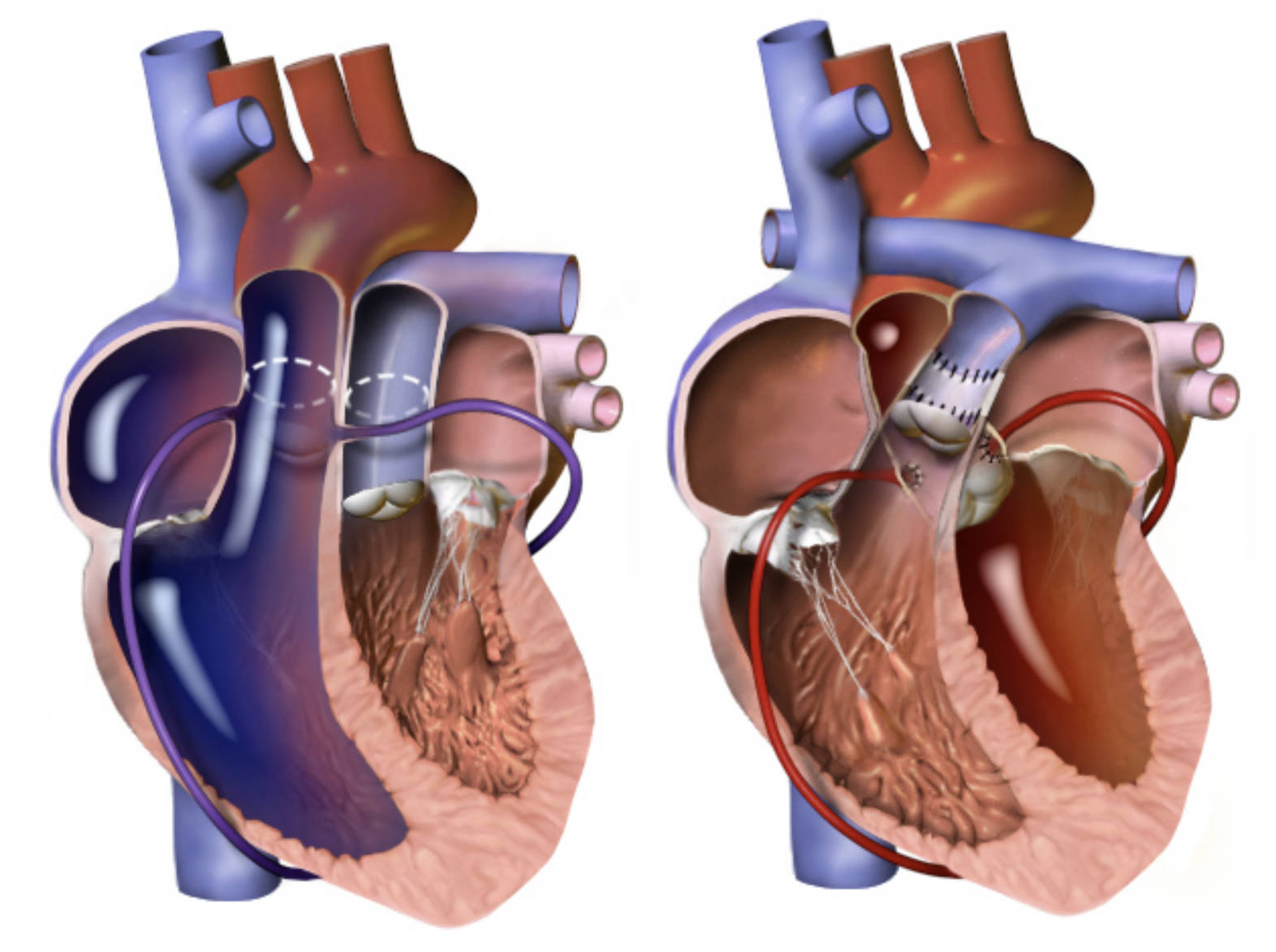
Pre-Operative Anatomy (Left Image): This illustration depicts the heart of an infant born with Transposition of the Great Arteries. Here, the aorta (the large vessel curving over the top) is incorrectly connected to the right ventricle, pumping deoxygenated (blue) blood back into the systemic circulation, while the pulmonary artery is connected to the left ventricle, sending oxygen-rich (red) blood back to the lungs inefficiently.
Post-Operative Correction (Right Image): This side shows the heart anatomy immediately following the arterial switch procedure. The surgeon has transected both great vessels and reattached them to their correct ventricles: the aorta is now connected to the left ventricle to distribute oxygenated blood, and the pulmonary artery is connected to the right ventricle to send blood to the lungs.
Coronary Artery Reimplantation: Visible as small vessels branching off the base of the aorta, the coronary arteries have been meticulously detached and transplanted. In the right-hand image, they are shown reattached to the “new” aorta (formerly the pulmonary root), ensuring the heart muscle receives oxygenated blood, a critical step for surgical success.
Vascular Anastomosis Sites: The suture lines visible on the great vessels in the right image indicate where the arteries were cut and reconnected. This reconstruction restores the normal hemodynamics of the heart, allowing the left ventricle to pump at systemic pressures and the right ventricle to pump at lower pulmonary pressures.
Understanding the Physiology of Transposition
Transposition of the Great Arteries (TGA) is a serious congenital heart defect that accounts for a significant percentage of cyanotic heart conditions in newborns. In a healthy heart, the circulation functions in a series: oxygen-poor blood flows to the lungs, picks up oxygen, and is pumped out to the body. In TGA, the reversal of the aorta and pulmonary artery creates two separate, parallel loops. One loop circulates oxygen-poor blood from the body back to the body, bypassing the lungs. The other loop circulates oxygen-rich blood from the lungs back to the lungs, never reaching the rest of the body.
Without surgical intervention, this anatomy is incompatible with life once the fetal shunts (like the ductus arteriosus and foramen ovale) close shortly after birth. The infant will present with severe cyanosis (blue tint to the skin) and dangerously low oxygen levels (hypoxia). The medical team must stabilize the infant, often using medication like prostaglandins to keep the fetal connections open, until surgery can be performed.
The Arterial Switch Operation (ASO), also known as the Jatene procedure, is the gold standard treatment for this condition. It is an anatomical repair, meaning it restores the heart to a normal structure rather than just rerouting blood flow (which was the goal of older atrial switch procedures). Key aspects of this medical intervention include:
- Timing: The surgery is typically performed within the first weeks of life, usually between day 3 and day 14.
- Coronary Transfer: Moving the tiny coronary arteries to the new aorta is the most technically demanding part of the surgery.
- Lecompte Maneuver: This surgical technique involves moving the pulmonary artery forward (anteriorly) to drape over the aorta, preventing vessel compression.
The Arterial Switch Operation Procedure
The primary goal of the Arterial Switch Operation is to establish a normal circulation pattern where the left ventricle pumps oxygenated blood to the aorta and the right ventricle pumps deoxygenated blood to the pulmonary artery. As illustrated in the provided image, the surgeon begins by transecting (cutting) both the aorta and the pulmonary artery just above the valves. The “roots” of the vessels (the parts attached to the heart) are left in place, but the tubes themselves are switched. The distal aorta is brought backward and connected to the left ventricular outflow tract (formerly the pulmonary root), and the pulmonary artery is brought forward and connected to the right ventricular outflow tract (formerly the aortic root).
A crucial component of this surgery involves the coronary arteries. In the pre-operative anatomy (left image), the coronary arteries originate from the vessel connected to the right ventricle (which is carrying deoxygenated blood). During the switch, the surgeon must excise the small “buttons” of tissue containing the coronary openings and reimplant them onto the new aorta (connected to the left ventricle). This ensures that the heart muscle itself receives red, oxygenated blood. If this step fails, the heart muscle will become ischemic and fail to pump effectively.
Prognosis and Long-Term Outcomes
Following a successful arterial switch, the outlook for children born with TGA is generally excellent. Because the left ventricle is anatomically designed to be the high-pressure pump for the body, restoring it to this role allows for normal development. Most children grow up with normal exercise tolerance and cardiac function. However, lifelong follow-up with a cardiologist is necessary to monitor for potential issues such as narrowing (stenosis) at the suture sites or dilation of the aortic root over time.
Conclusion
The illustration highlights the remarkable surgical engineering required to correct Transposition of the Great Arteries. By physically switching the major outflow tracts and carefully reimplanting the coronary arteries, the arterial switch operation converts a fatal anatomy into a functional, normal heart. This procedure stands as a major triumph in pediatric cardiac surgery, allowing infants who would otherwise not survive to lead healthy, active lives.


{kind=link}