Explore the crucial differences in oxygen-hemoglobin dissociation curves between fetal and adult hemoglobin, highlighting the remarkable adaptation that ensures efficient oxygen transfer to the developing fetus. This article delves into how fetal hemoglobin’s higher oxygen affinity is essential for intrauterine survival.
The Marvel of Maternal-Fetal Oxygen Transfer
The journey from conception to birth is a complex physiological marvel, with oxygen delivery being one of the most critical aspects for fetal development. Unlike adults who breathe air directly, a fetus relies entirely on the mother for its oxygen supply, which must be efficiently transferred across the placenta. This intricate process is made possible by a remarkable biochemical adaptation: the presence of different types of hemoglobin in the fetus compared to the adult. The distinct properties of fetal and adult hemoglobin are elegantly illustrated by their respective oxygen-hemoglobin dissociation curves.
Understanding the unique characteristics of fetal hemoglobin (HbF) and how its oxygen affinity differs from adult hemoglobin (HbA) is fundamental in perinatal medicine. This specialized adaptation ensures that the fetus can effectively “pull” oxygen from the maternal bloodstream, a vital mechanism for sustaining growth and development in a relatively low-oxygen intrauterine environment.
Key distinctions in oxygen transport include:
- Fetal hemoglobin’s higher affinity for oxygen.
- Efficient oxygen transfer across the placenta.
- Adaptation to a hypoxic intrauterine environment.
These differences are crucial for successful fetal development.
The Oxygen-Hemoglobin Dissociation Curves: Fetal vs. Adult
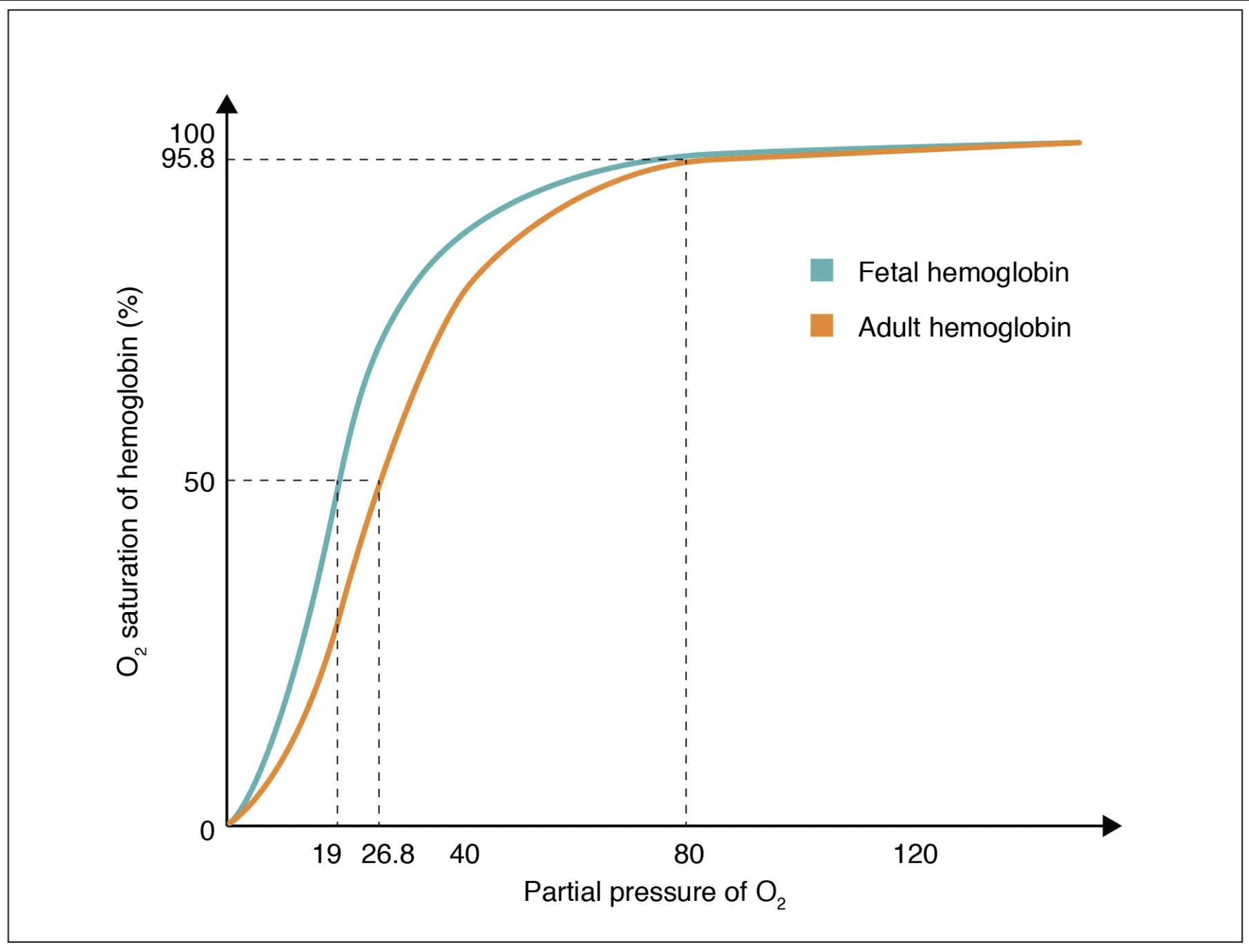
The oxygen-hemoglobin dissociation curve plots the percentage of hemoglobin saturated with oxygen against the partial pressure of oxygen (PO2). This graph visually represents how readily hemoglobin binds to and releases oxygen. The image showcases two distinct curves, highlighting the crucial difference in oxygen affinity between fetal and adult hemoglobin.
O2 saturation of hemoglobin (%): This vertical axis indicates the percentage of hemoglobin molecules that are currently bound to oxygen. A higher percentage means more oxygen is being carried.
Partial pressure of O2 (mm Hg): This horizontal axis represents the partial pressure of oxygen, the driving force for oxygen to bind to or dissociate from hemoglobin. Higher partial pressures, as found in the lungs, promote oxygen loading.
Fetal hemoglobin: Represented by the blue curve, fetal hemoglobin (HbF) demonstrates a significantly higher affinity for oxygen compared to adult hemoglobin. This leftward shift of the curve means that at any given partial pressure of oxygen, fetal hemoglobin will be more saturated with oxygen than adult hemoglobin.
Adult hemoglobin: Represented by the orange curve, adult hemoglobin (HbA) has a lower affinity for oxygen than fetal hemoglobin. Its curve is shifted to the right relative to the fetal curve, indicating that it releases oxygen more readily at a given PO2.
The Physiological Advantage of Fetal Hemoglobin
The most striking difference between fetal and adult hemoglobin lies in their respective affinities for oxygen. As clearly depicted by the leftward shift of the blue curve, fetal hemoglobin has a greater affinity for oxygen than does adult hemoglobin. This physiological advantage is critical for the fetus, which exists in a relatively hypoxic environment within the womb, receiving oxygenated blood from the placenta where the PO2 is lower than in the adult lungs.
At the placenta, maternal blood (containing adult hemoglobin) has a certain PO2. Due to the higher affinity of fetal hemoglobin for oxygen, it can effectively “extract” oxygen from the maternal blood. This means that at the same PO2, fetal hemoglobin will be more saturated with oxygen than maternal adult hemoglobin. For instance, at a placental PO2 of approximately 20-30 mm Hg, fetal hemoglobin can achieve significantly higher saturation levels (e.g., 50% saturation at ~19 mm Hg) compared to adult hemoglobin (50% saturation at ~26.8 mm Hg). This difference ensures that despite the lower oxygen tension in the placenta, the fetus receives an adequate supply of oxygen for its rapid growth and development.
Molecular Basis and Clinical Significance
The difference in oxygen affinity between fetal and adult hemoglobin is due to their distinct protein structures. Adult hemoglobin (HbA) is composed of two alpha and two beta globin chains, whereas fetal hemoglobin (HbF) consists of two alpha and two gamma globin chains. The gamma chains in HbF have a reduced interaction with 2,3-bisphosphoglycerate (2,3-BPG), a molecule that decreases hemoglobin’s affinity for oxygen. Because HbF binds 2,3-BPG less effectively, its affinity for oxygen remains higher, allowing it to efficiently draw oxygen from the maternal circulation across the placental barrier.
Clinically, this differential affinity is crucial. Conditions that compromise placental blood flow or maternal oxygenation can significantly impact fetal oxygen supply. Understanding the fetal oxygen-hemoglobin dissociation curve helps clinicians assess fetal well-being and manage complications during pregnancy. After birth, as the infant begins to breathe air and is exposed to a higher PO2 environment, the production of fetal hemoglobin gradually decreases, and adult hemoglobin production increases, adapting the infant’s oxygen transport system to extrauterine life over the first few months.
Conclusion
The unique oxygen-hemoglobin dissociation curve of fetal hemoglobin, exhibiting a greater affinity for oxygen than adult hemoglobin, represents a remarkable evolutionary adaptation for intrauterine survival. This physiological distinction ensures efficient oxygen transfer from the mother’s blood across the placenta to the developing fetus, providing the critical oxygen supply needed for growth and metabolic activity. A thorough understanding of these differences is indispensable in obstetrics and neonatology, enabling healthcare professionals to monitor fetal oxygenation and manage conditions that may compromise this vital exchange, ultimately safeguarding the health of both mother and child.


{kind=link}